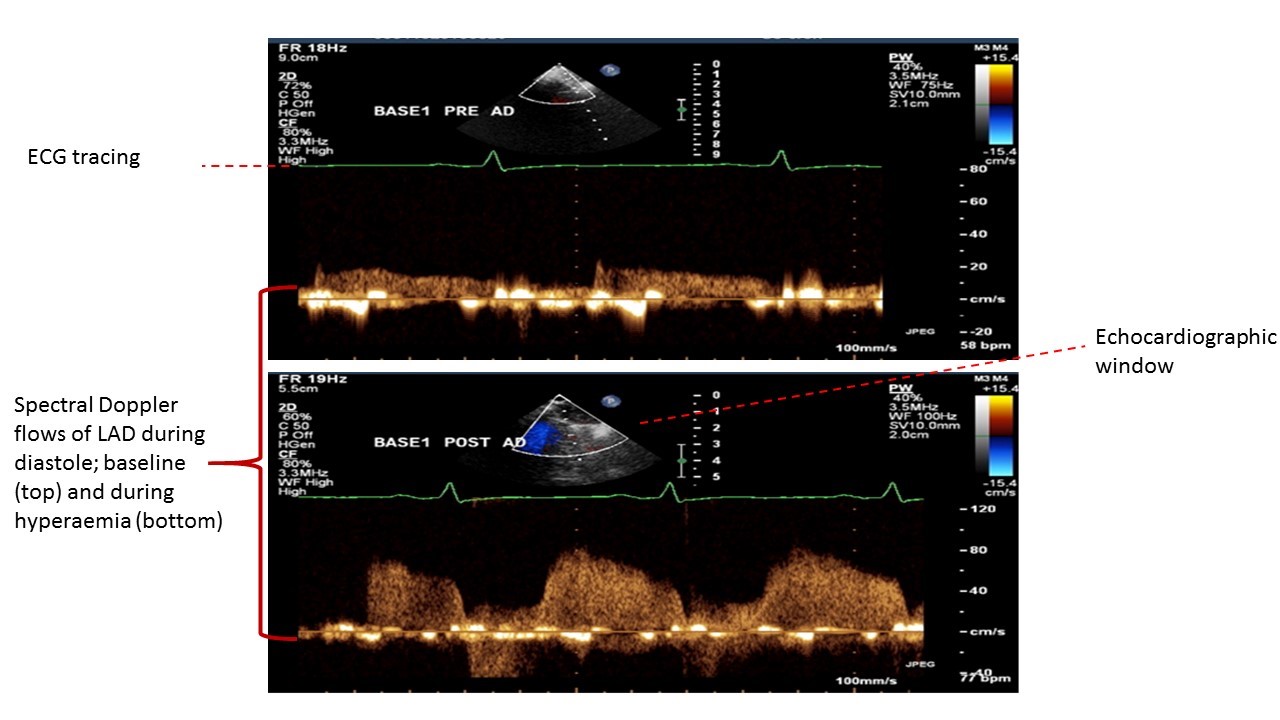
The present study used a well validated, non-invasive method to examine the effect of acute hypoglycemia on real-time coronary arterial flow in adults with and without type 1 diabetes, with the coronary flow ratio (CFR) being measured using transthoracic Doppler echocardiography. During acute hypoglycemia, young adult males with type 1 diabetes had a trend of lower coronary flow reserve compared with an age-matched group of non-diabetic males. The modest decline in CFR was well tolerated in young men with type 1 diabetes who were otherwise healthy and had no evidence either of microvascular complications or of coronary heart disease; normal coronary reserve was maintained.
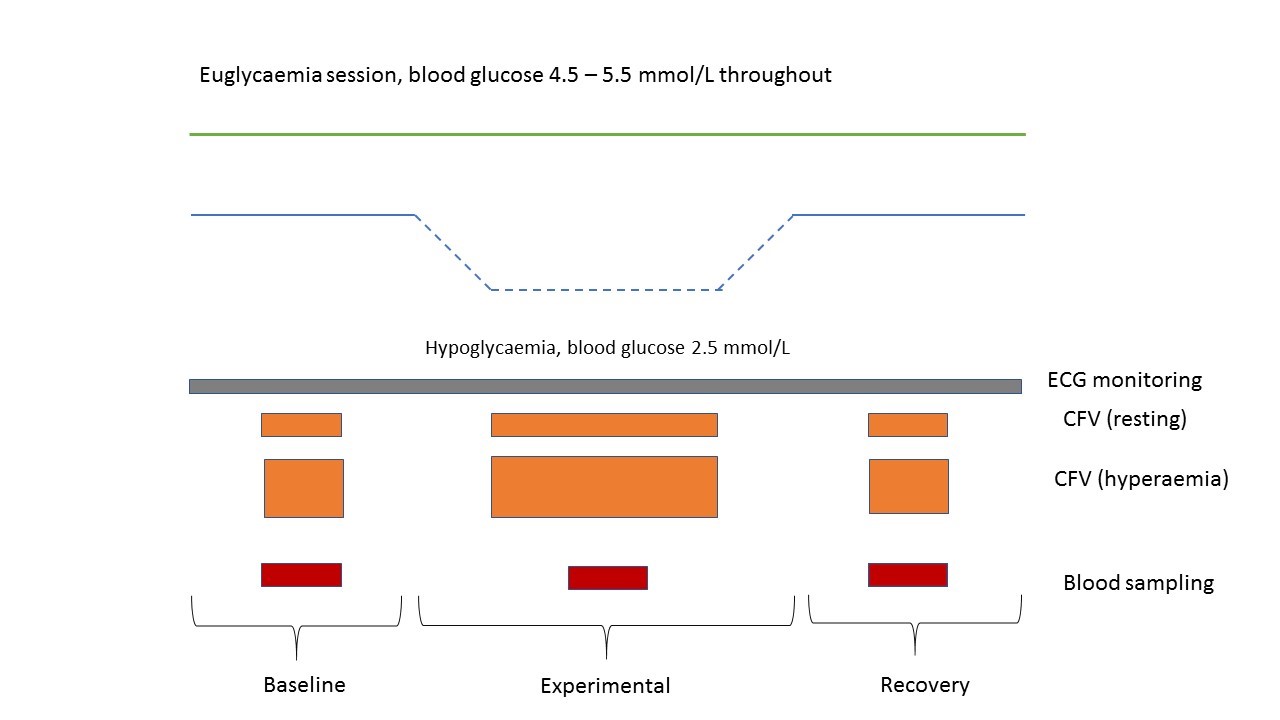
The direct effects of hypoglycemia on cardiac function have proved difficult to elucidate as insulin per se exerts direct effects on the heart. Fisher et al (9) showed that administration of insulin caused an immediate increase in left ventricular ejection fraction and provoked sympathetic activation, both of which occurred before any fall in blood glucose. As blood glucose declined progressively, these responses became more pronounced, with the maximal changes coinciding with the glucose nadir (9). A strength of the present study was the ability to use a non-invasive real-time assessment of coronary flow reserve during acute hypoglycemia. By using a hyperinsulinemic glucose clamp it was possible to compare CFR during euglycemia and hypoglycemia, and between type 1 diabetes and the non-diabetic state. The changes observed are therefore related to the low blood glucose and to counterregulatory mechanisms, and not to the intravenous infusion of insulin per se. Furthermore, this study provides a direct assessment of coronary vasomotor function which excludes other potential confounders such as hypertension or microvascular disease.
The main limitation of the study is the small sample size. While this was in part a consequence of the robust exclusion criteria, the demanding study design also limited recruitment of potential participants, specifically because of the use of adenosine to induce maximal hyperemia of the coronary blood vessels. The rationale for using adenosine was its short half-life, which meant that the CFR values from one measurement to the next would not be confounded by residual effects of adenosine. The disadvantage of this approach is that adenosine is often poorly tolerated because it induces unpleasant side-effects of chest tightness and facial flushing, which diminishes the willingness of volunteers to participate. In addition, the glucose clamp procedure is onerous and had to be repeated at least two weeks apart, which was a further limitation to recruitment.
In retrospect, the power calculation may have benefited from an a priori calculation of possible attrition of participants, or non-concordance with the protocol. Additionally, the magnitude of the primary outcome (difference of 0.57 in CFR) may have been over-ambitious, given that our participants with diabetes were fit and in good health. In view of the relatively small sample size of our study, it is possible that we did not have sufficient power to detect a significant interaction between diabetes status and experimental condition in the generalised linear mixed model analysis. Therefore, while this study models the direct effect of hypoglycemia per se on coronary vasomotor function, the generalisability of the results must take into account the sample size and the exclusion of female participants.
A previous investigation by Rana and colleagues (32), which to our knowledge is the only other study to have explored the effect of acute hypoglycemia on the myocardial circulation, used sequential hyperinsulinemic glucose clamps and dipyridamole-induced stress echocardiography to measure myocardial blood flow reserve during euglycemia and acute hypoglycemia in adults of both sexes, 28 with, and 19 without type 1 diabetes (32). The age range was wider than in the present study and included people with microvascular disease. Hypoglycemia induced a significant fall in myocardial blood flow reserve in both groups, with lower values being observed in the group with type 1 diabetes at all times of measurement. A statistically significant association was observed with the presence of microvascular complications. In contrast to the present study design, no time interval was allowed between the initial euglycemia and the subsequent induction of hypoglycemia, so that myocardial blood flow reserve rose during the period of protracted euglycemia, which may have influenced the effect on the subsequent hypoglycemia (32). In addition, the order of the euglycemic and hypoglycemic clamps was not randomized, which may have introduced observer bias and an order effect. Furthermore, the long half-life of dipyridamole might have influenced the results. The present study may therefore have provided a more direct model of coronary flow reserve with fewer confounding factors such as the presence of microvascular disease and a possible residual effect of dipyridamole.
In the present study no significant change in CFR was observed during hypoglycemia. While a non-significant trend towards a lower CFR was observed in the participants with type 1 diabetes during euglycemia, a trend towards a decline in CFR was also observed during hypoglycemia, consistent with previous observations (17). The lowest CFR values during hypoglycemia were observed in the participants with type 1 diabetes. The increments in heart rate and systolic blood pressure in the group with type 1 diabetes did not achieve statistical significance (Table 2), which was unexpected with this degree of hypoglycemia. The small sample size may not have allowed sufficient sensitivity to detect small variations in pulse and blood pressure. An alternative interpretation is that some participants with type 1 diabetes may have had some degree of autonomic dysfunction or a diminished catecholamine response to hypoglycemia, which contributed to the modest hemodynamic changes and the lower CFR values observed in the group with type 1 diabetes. As formal assessment of autonomic function in the participants was not made nor were plasma catecholamines measured, this possibility cannot be excluded.
A Danish study using non-invasive cardiac magnetic resonance imaging has reported that myocardial blood flow reserve was higher at rest and lower during vasodilatory stress in people with type 2 diabetes compared with non-diabetic controls (33). Impaired myocardial blood flow reserve was associated with microvascular complications (albuminuria and retinopathy) of diabetes. The present study explicitly excluded people with overt microvascular disease; it is possible that the development of cardiac microangiopathy may underlie an abnormal response to hypoglycemia in type 1 diabetes (33).
While no change in the highly sensitive troponin values was observed during acute hypoglycemia, this was measured in close temporal proximity to the blood glucose nadir. It is possible that measurement in the immediate ‘recovery’ stage was made too early to detect a rise in plasma troponin and exclude evidence of myocardial insult.
The results of the present study imply that any putative cardiac harm of hypoglycemia is unlikely to be mediated solely through coronary vasomotor dysfunction. Other potentially harmful factors associated with hypoglycemia may be required, such as the promotion of pro-thrombotic mechanisms (34, 35), endothelial abnormalities (11), or altered cardiac electrical conduction (36, 37),. It should also be noted that this study specifically studied acute hypoglycemia, and the cumulative effects of recurrent hypoglycemia have not been examined.
Recent randomized controlled trials (RCTs) that did not target strict glycemic control but used drugs with a low risk of hypoglycemia have shown beneficial cardiovascular outcomes (38, 39). This is in direct contrast to previous RCTs, in which very strict glycemic control was pursued and the incidence of severe hypoglycemia was high (10). These findings suggest that avoidance of hypoglycemia is important to achieve cardiovascular benefit.
{kind=link}
{kind=link}