Aim
To determine the feasibility of implementing the MOEWS tool in the setting of obstetric ICU
Setting
Department of Obstetrics and Gynecology, West China Women's and Children's Hospital of Sichuan University is one of the first national key clinical specialty construction, and it is the treatment and referral center of severe pregnant women in western China that conducts about 16,000 deliveries annually.
Study Design
This was a retrospective study implemented in our hospital from August 2019 to August 2020. A total of 19,438 deliveries occurred during the study period. There were 378 obstetric patients admitted to the dedicated obstetric ICU. All obstetric patients were pregnant and postpartum women within 42 days of delivery, and patients with an ICU stay of at least 24 hours were enrolled. Because multiple patients were in critical condition before ICU admission, we assessed the MOEWS 24 hours before and 24 hours after admission to the ICU, and the highest score was taken as the final value. In addition, the APACHE II score was calculated within 24 hours of ICU admission. For calculation of the score, the most abnormal reading of each clinical and laboratory parameter was considered.
The parameters and their numerical values used for the calculation of the MOEWS are shown in Table 1. Measurements of temperature, respiratory rate, and peripheral oxygen saturation, the method of oxygen therapy (nasal catheters, mask, noninvasive ventilator, invasive ventilator), heart rate, blood pressure, and consciousness level (alert, responding to sound or pain and unresponsive) were documented. Regarding the APACHE II score, all laboratory parameters were obtained through venous blood sampling. The partial pressure of oxygen (PaO2) in arterial blood (in mmHg) was recorded from the arterial blood gas (ABG) analysis.
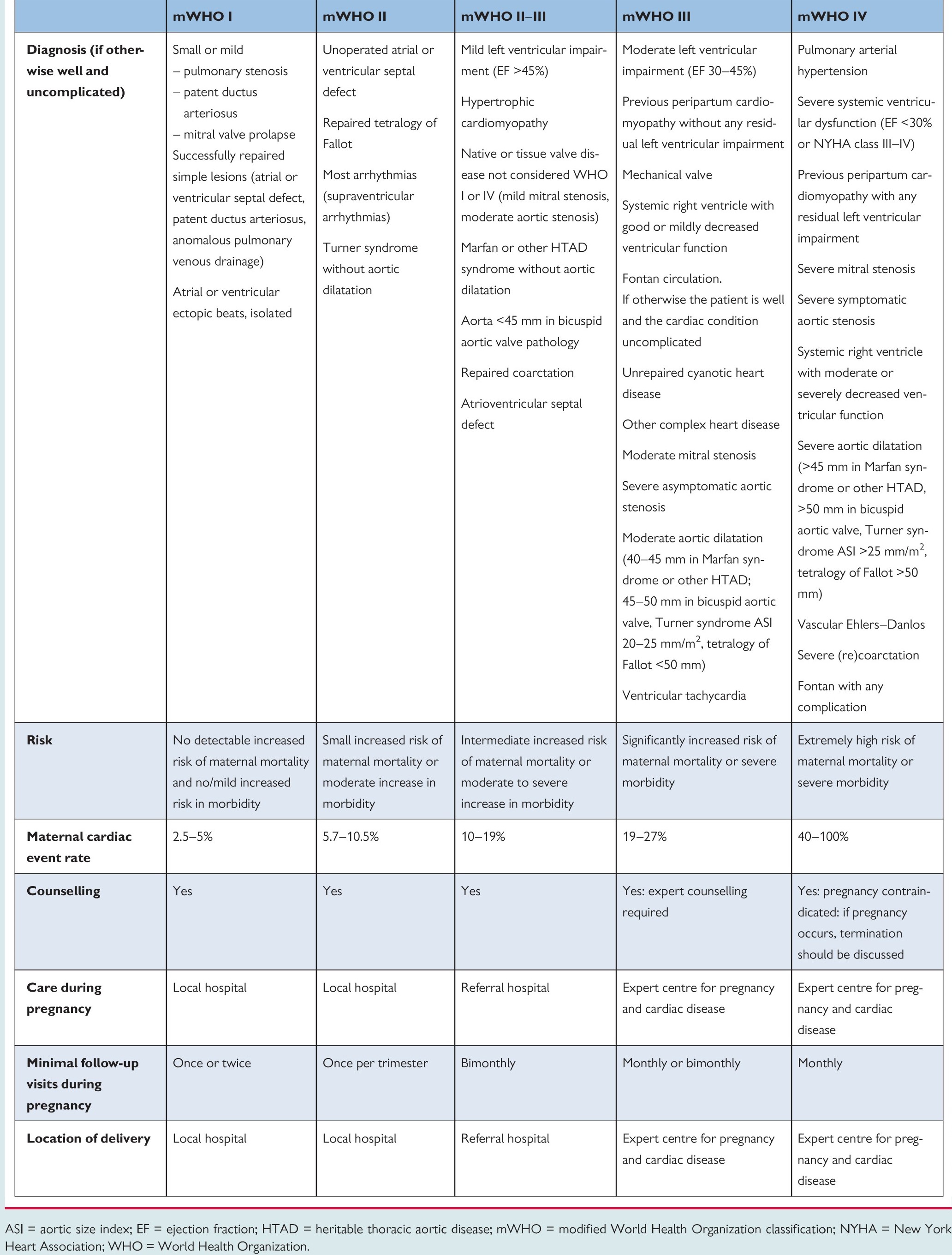
Hypertensive disorders in pregnancy, postpartum haemorrhage and pregnancy with heart diseases constitute the main causes of maternal death[24–27]. Women with severe hypertension who underwent treatment with intravenous antihypertensive agents were considered critically ill[28, 29]. Additionally, maladaptation of the cardiovascular system during pregnancy can lead to complications that may put the mother at risk of developing cardiac dysfunction and subsequent heart failure[30]. Consequently, the modified World Health Organization (mWHO) classification of maternal cardiovascular risk was used to assess the maternal risk of cardiac complications(Attached table1). In this study, patients with cardiovascular diseases whose mWHO risk classification was III or IV were identified as high-risk women[31].
Notably, the vital signs indicating postpartum haemorrhage and cardiac disease were not significantly abnormal in the early stages in many pregnant women, in spite of the vast potential risks for these patients. As a result, 3 points was added to the MOEWS in women confirmed to have severe postpartum haemorrhage or high-risk cardiovascular disease. The definition of severe postpartum haemorrhage was shown in Table 2.
Table 1. Cut-off limits of individual parameters for the MOEWS

Recommended clinical reaction: The critical care system changes colour based on the score of each parameter to alert the ICU team to initiate a clinical response, with scores of 3 turning red and 2 turning yellow. When the total MOEWS ≤ 2, the current plan is maintained; when the MOEWS =3–4, the observations are repeated; when the MOEWS ≥5 or a single parameter score is ≥3, the patient is admitted to the ICU. *The details were shown in Table 2 and the attached table1.
The study endpoint was severe maternal morbidity, while the secondary outcomes were the length of ICU stay, age, gestational age, the number of requirements for ventilation, vasopressors, intravenous antihypertensive drugs, transfusion, hysterectomy, arterial embolization, haemodialysis and extracorporeal membrane oxygenation (ECMO). The relative definitions of maternal morbidity are shown in Table 2.
Table 2: Diagnostic criteria of severe obstetric morbidity
|
Obstetric morbidity
|
Diagnostic criteria
|
|
Pre-eclampsia[19]
|
SBP≥160 mmHg, or DBP ≥ 110 mmHg plus proteinuria ≥ 0.3 g. day-1 (+2 dipstick) or hypertension (≥140/90 mmHg) and proteinuria with at least one of the following: headache; visual disturbance; epigastric pain; clonus; platelet count ≤100 .109 -1); AST >50 iu.l-1; Cr > 100 umol.l -1; or CrCl < 80.8 ml.min-1
|
|
Eclampsia[29]
|
Severe preeclampsia characterized by sudden onset of generalized tonic-clonic seizures
|
|
Obstetric haemorrhage[19]
|
Documented estimated blood loss ≥1500 ml, drop in haemoglobin concentration >3 g/dl or need for blood transfusion
|
|
Severe postpartum haemorrhage[14, 32]
|
Documented estimated blood loss ≥2000 ml, need for blood transfusion of at least 3 U, or hysterectomy, with or without radiological embolization of uterine arteries
|
|
Suspected infection[19]
|
Clinically suspected focus of infection ± positive laboratory culture, treated with antibiotics (excluding commensals and antibiotic prophylaxis)
|
|
Shock[18]
|
Persistent severe hypotension defined as systolic blood pressure <90 mmHg for 60 min or decreased by 40 mmHg
|
|
Pulmonary oedema[19]
|
Breathlessness, crepitation requiring diuretics
|
|
Thromboembolism[12]
|
CTPA confirmed pulmonary embolism, venous thrombosis in the pelvic region, deep venous thrombosis in the extremities or sinus thrombosis
|
|
Diabetic ketoacidosis[19]
|
Hyperglycaemia, metabolic acidosis, ketones in urine
|
|
Intracranial tumour[19]
|
CT ⁄ MRI confirmed
|
|
Status epilepticus[19]
|
History of epilepsy, prolonged multiple seizures
|
|
Other serious medical conditions[19, 33–35]
|
Acute pancreatitis, liver failure, acute fatty liver of pregnancy, acute appendicitis or other critical illness
|
SBP, systolic blood pressure; DBP, diastolic blood pressure; AST, aspartate aminotransferase; Cr, creatinine; CrCL, creatinine clearance; CTPA, computed tomography pulmonary angiogram; MRI, magnetic resonance imaging.
Statistical analysis
The results were tabulated and subjected to statistical analysis using Statistical Package for Social Sciences (SPSS) version 25.0. ROC curves were used to determine the area under the curve of various scores for predicting severe morbidity. Sensitivity, specificity, positive predictive values (PPVs), and negative predictive values (NPVs) were calculated. For all statistical tests, we regarded a value of p < 0.05 as statistically significant.
{kind=link}