Baseline Characteristics of the Study Population
Of the 3,465 screened patients, 461 patients were enrolled for analysis and classified into three group as follows: low-PA (n = 171), moderate-PA (n = 149), and high-PA (n = 141) groups (Fig. 1). The baseline characteristics are shown in Table 1. No significant differences were observed among the three groups in terms of demographic characteristics, admission category, and illness severity parameters. Almost half of the patients were admitted to the ICU for reasons such as respiratory failure, pneumonia, and septic shock. The most common comorbid condition was malignancy. Patients in the high-PA group were more likely to have respiratory disease (P < 0.01). The details of respiratory disease were as follows: chronic obstructive pulmonary disease (COPD), 42%; interstitial lung disease, 31.8%; bronchial asthma, 21.6%; bronchiectasis, 12.5%. Laboratory findings at ICU admission showed that patients in the high-PA group had significantly higher mean blood glucose levels and more hyperglycemia than other groups (P < 0.01).
Table 1
Patient’s characteristics at ICU admission
| | Low-PA group (n = 171) | Moderate-PA group (n = 149) | High-PA group (n = 141) | P-value |
| Age, median (IQR), years | 66 (57‒74) | 66 (56‒76) | 67 (56‒77) | 0.81 |
| Sex, female | 58 (33.9%) | 50 (33.6%) | 54 (38.3%) | 0.64 |
| Admission category | | | | 0.15 |
| Medical | 86 (50.3%) | 82 (55%) | 83 (58.9%) | |
| Elective surgery | 52 (30.4%) | 30 (20.1%) | 34 (24.1%) | |
| Emergency Surgery | 33 (19.3%) | 37 (24.8%) | 24 (17%) | |
| Main reason for ICU admission | | | | |
| Respiratory failure | 47 (27.5%) | 35 (23.5%) | 35 (24.8%) | 0.7 |
| Pneumonia | 28 (16.4%) | 17 (11.4%) | 21 (14.9%) | 0.44 |
| Septic shock | 22 (12.9%) | 15 (10.1%) | 19 (13.5%) | 0.63 |
| Neurological failure | 14 (8.2%) | 17 (11.4%) | 12 (8.5%) | 0.57 |
| Severity parameter, median (IQR) | | | | |
| APACHE II | 22 (17‒28) | 22 (18‒28) | 22 (19‒28) | 0.57 |
| SOFA | 9 (6‒12) | 10 (7‒12) | 9 (6‒12) | 0.27 |
| Main comorbidities | | | | |
| Malignant disease | 62 (36.3%) | 53 (35.6%) | 59 (41.8%) | 0.48 |
| Cardiovascular disease | 58 (33.9%) | 47 (31.5%) | 43 (30.1%) | 0.8 |
| Neurologic disease | 54 (31.6%) | 39 (26.2%) | 35 (24.8%) | 0.36 |
| Diabetes mellitus | 36 (21.1%) | 26 (17.5%) | 31 (22%) | 0.59 |
| Respiratory disease | 37 (21.6%) | 17 (11.4%) | 34 (24.1%) | < 0.01 |
| Immunosuppression | 33 (19.3%) | 20 (13.4%) | 30 (21.3%) | 0.19 |
| Charlson comorbidity index, median (IQR) | 6 (4‒8) | 6 (4‒7) | 6 (4‒7) | 0.72 |
| Events prior to ICU admission | | | | |
| Prior colonization or infection with P. aeruginosa | 39 (22.8%) | 25 (16.9%) | 30 (21.3%) | 0.41 |
| Surgery within 30 days | 91 (53.2%) | 83 (55.7%) | 78 (55.3%) | 0.89 |
| Hospitalization within 1 year | 105 (61.4%) | 86 (57.7%) | 82 (58.2%) | 0.76 |
| Laboratory findings, median (IQR) | | | | |
| Mean blood glucose during first 24 h (mg/dL) | 137 (113‒165) | 145 (112‒173) | 157 (125‒198) | < 0.01 |
| Hyperglycemia | 38 (22.2%) | 39 (26.2%) | 60 (42.6%) | < 0.01 |
| WBC (/µL) | 11,000 (8,100‒15,600) | 11,700 (8,950‒15,850) | 12,500 (8,900‒21,780) | 0.18 |
| CRP (mg/dL) | 7.7 (3.4‒16.5) | 8.5 (1.6‒18.3) | 7.3 (3.6‒17.1) | 0.73 |
| Albumin (g/dL) | 2.5 (2.1‒3) | 2.6 (2.2‒3) | 2.4 (2.1‒2.9) | 0.21 |
| APACHE Acute Physiology and Chronic Health Evaluation, CRP C-reactive protein, ICU intensive care unit, IQR interquartile range, PA Pseudomonas aeruginosa, SOFA Sequential Organ Failure Assessment score, WBC white blood cell |
Clinical Features And Outcomes
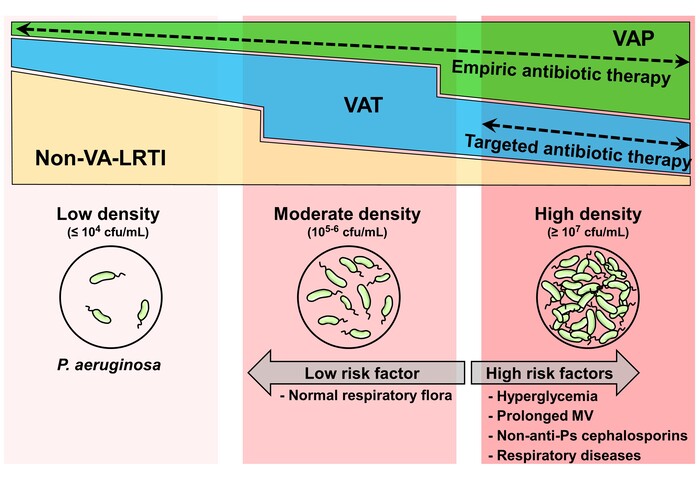
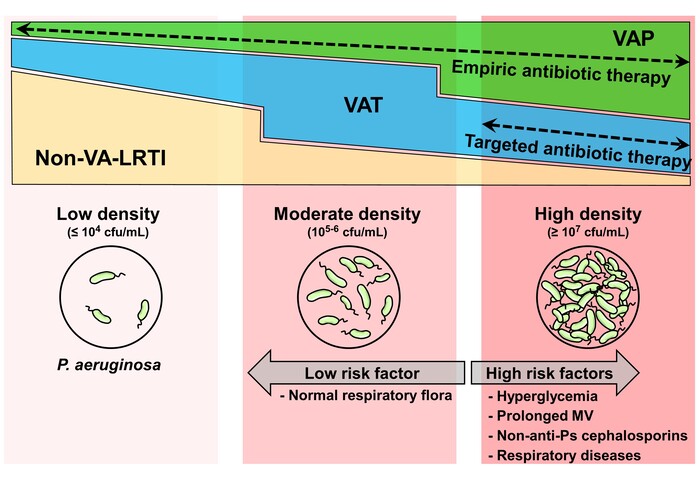
The clinical features at the time-point when the peak density of PA was detected are presented in Table 2. The frequency of VA-LRTI was less than 50% in the low-PA group, whereas it was about 80% in the moderate- and high-PA group. VAT accounted for about 70‒80% of VA-LRTI in each group, and the frequency of VAP tended to be higher in high-PA group (P < 0.01). SOFA scores did not differ significantly among the three groups, whereas the CPIS tended to increase as the PA density increased. Levels of systemic inflammation markers, including white blood cell (WBC) count and C-reactive protein (CRP), were also higher in the high-PA group than in other groups (P < 0.01). Chest X-rays showed that pulmonary infiltrate lesions were more diffuse in the high-PA group.
Table 2
Patients’ characteristics at time of peak density of Pseudomonas aeruginosa isolation from endotracheal aspirates
| | Low-PA group (n = 171) | Moderate-PA group (n = 149) | High-PA group (n = 141) | P-value |
| VA-LRTI | | | | < 0.01 |
| Non-VA-LRTI | 95 (55.6%) | 34 (22.8%) | 25 (17.7%) | |
| VAT | 60 (35.1%) | 96 (64.4%) | 81 (57.5%) | |
| VAP | 16 (9.4%) | 19 (12.8%) | 35 (24.8%) | |
| Length of MV, median (IQR), days | 5 (2‒13) | 11 (5‒20) | 10 (4‒24) | < 0.01 |
| SOFA | 7 (5‒11) | 8 (5‒11) | 8 (5‒12) | 0.51 |
| CPIS | 3 (2‒5) | 4 (3‒5) | 5 (3‒6) | < 0.01 |
| Chest X-ray findings | | | | 0.02 |
| No infiltrate | 84 (49.1%) | 61 (40.9%) | 44 (31.2%) | |
| Unilateral infiltrates | 58 (33.9%) | 65 (43.6%) | 66 (46.8%) | |
| Bilateral infiltrates | 29 (17%) | 23 (15.4%) | 31 (22%) | |
| Laboratory findings, median (IQR) | | | | |
| WBC (/µL) | 10900 (7600‒13300) | 9800 (6450‒13450) | 12110 (7950‒16600) | < 0.01 |
| CRP (mg/dL) | 7.5 (3.3‒14.1) | 5.7 (2.5‒9.7) | 8.2 (2.9‒16) | < 0.01 |
| Albumin (g/dL) | 2.6 (2.2‒2.9) | 2.6 (2.2‒2.9) | 2.5 (2‒2.8) | 0.11 |
| Tracheal aspirates analysis | | | | |
| Neutrophil counts | | | | < 0.01 |
| 0 to 1+ | 47 (27.5%) | 23 (15.4%) | 27 (19.2%) | |
| 2 + to 3+ | 74 (43.3%) | 60 (40.3%) | 42 (29.8%) | |
| 4+ | 50 (29.2%) | 66 (44.3%) | 72 (51.1%) | |
| Culture results | | | | |
| Normal respiratory flora | 96 (56.1%) | 68 (45.6%) | 55 (39%) | < 0.01 |
| Candida sp. | 46 (26.9%) | 46 (30.9%) | 42 (29.8%) | 0.72 |
| Staphylococcus aureus | 29 (17%) | 20 (13.4%) | 21 (14.9%) | 0.67 |
| Stenotrophomonas maltophilia | 32 (18.7%) | 20 (13.4%) | 13 (9.2%) | 0.054 |
| Klebsiella pneumoniae | 10 (5.6%) | 13 (8.7%) | 10 (7.1%) | 0.61 |
| Clinical outcomes | | | | |
| VFDs at 28 days | | | | |
| Median (IQR), days | 24 (6‒27) | 21 (0‒27) | 1 (0‒24) | < 0.01 |
| Adjusted coefficient B (95% CI)a | reference | 1.1 (-0.2 to 2.42) | ‒1.94 (-3.28 to -0.61) | 0.1b, < 0.01c |
| ICU mortality | | | | |
| No. of cases | 17 (9.9%) | 22 (14.8%) | 36 (25.3%) | < 0.01 |
| Adjusted OR (95% CI)a | reference | 1.27 (0.46‒3.54) | 2.78 (1.02‒7.58) | 0.64b, 0.047c |
| CI confidence interval, CPIS Clinical Pulmonary Infection Score, CRP C-reactive protein, ICU intensive care unit, IQR interquartile range, MV mechanical ventilation, OR odds ratio, PA Pseudomonas aeruginosa, SOFA Sequential Organ Failure Assessment score, WBC white blood cell, VA-LRTI ventilator-associated lower respiratory tract infection, VAP ventilator-associated pneumonia, VAT ventilator-associated tracheobronchitis, VFDs ventilator-free days |
| aAdjusted for age, sex, respiratory diseases, APACHE II at ICU admission, presence of VAT or VAP, length of MV and SOFA when maximum density of PA was detected. |
| bModerate PA density vs. Low PA density. |
| cHigh PA density vs. Low PA density. |
In the analysis of ETA, the number of neutrophil cells increased as the PA density increased (P < 0.01). Regarding pathogenic bacteria besides PA, counts of Stenotrophomonas maltophilia were slightly lower in the high-PA group. VFDs at 28 days and ICU mortality were worse in the higher density groups.
After adjustment by multivariate analysis, the high-PA group still had significantly worse clinical outcomes than the low-PA group (VFDs, Adjusted coefficient B ‒1.94, 95% confidence intervals [CI] ‒3.28 to ‒0.61, P < 0.01; ICU mortality, odds ratio [OR] 2.78, 95%CI 1.02‒7.58, P = 0.047), whereas the moderate-PA group did not differ significantly from the low-PA group.
Risk Factors for High Density of Pseudomonas aeruginosa in Airway
Table 3 presents risk factors associated with high-PA in univariate and multivariate analyses. Univariate logistic regression analysis revealed that longer duration (> 28 days) of MV, hyperglycemia, and use of non-antipseudomonal cephalosporins during the ICU stay were all significantly associated with high-PA in MV patients. Patients with NRF during their ICU stay had a lower risk of having high-PA. The main microorganisms in the NRF were Candida sp. (34.1%), α-Streptococcus sp. (29.7%), and coagulase-negative staphylococci (14.3%). Marginal associations were observed for respiratory disease, low serum albumin levels at ICU admission, and use of antifungal antibiotics during the ICU stay.
Table 3
Risk factors for high-density Pseudomonas aeruginosa isolation during ICU stay
| | Univariate | P-value | Multivariate | P-value |
| | OR (95% CI) | OR (95% CI) |
| Characteristics at ICU admission | | | | |
| Age | 1.0 (0.99‒1.01) | 0.79 | | NS |
| Female sex | 1.22 (0.81‒1.84) | 0.35 | | NS |
| Respiratory diseases | 1.57 (0.96‒2.54) | 0.069 | 1.9 (1.12‒3.23) | 0.02 |
| Albumin (g/dL) | 0.79 (0.57‒1.09) | 0.15 | | NS |
| APACHE II | 1.01 (0.98‒1.03) | 0.58 | | NS |
| Events prior to peak density of P. aeruginosa isolation | | | | |
| Length of mechanical ventilation | | | | |
| ≤7 days | reference | | | |
| 8‒14 days | 1.23 (0.73‒2.07) | 0.44 | | NS |
| 15‒21 days | 0.75 (0.37‒1.53) | 0.43 | | NS |
| 22‒28 days | 1.23 (0.55‒2.74) | 0.61 | | NS |
| >28 days | 3.16 (1.7‒5.9) | < 0.01 | 3.07 (1.35‒6.97) | < 0.01 |
| Hyperglycemia | 1.9 (1.27‒2.84) | < 0.01 | 2.01 (1.26‒3.22) | < 0.01 |
| Bacteria isolated in tracheal aspirates | | | | |
| Normal respiratory flora | 0.52 (0.32‒0.84) | < 0.01 | 0.43 (0.26‒0.73) | < 0.01 |
| Stenotrophomonas maltophilia | 1.56 (0.76‒3.18) | 0.22 | | NS |
| Antibiotic therapy | | | | |
| Non-antipseudomonal cephalosporins | 1.78 (1.16‒2.72) | < 0.01 | 2.17 (1.35‒3.49) | < 0.01 |
| Antipseudomonal antibiotics | 1.11 (0.74‒1.65) | 0.61 | | NS |
| Antifungal antibiotics | 1.51 (0.95‒2.39) | 0.08 | | NS |
| APACHE Acute Physiology and Chronic Health Evaluation, CI confidence interval, NS not significant, OR odds ratio, P. aeruginosa Pseudomonas aeruginosa |
Multivariate logistic regression analysis confirmed that independent risk factors for high-PA were longer duration (> 28 days) of MV (OR 3.07, 95%CI 1.35‒6.97, P < 0.01), use of non-antipseudomonal cephalosporins (OR 2.17, 95% CI 1.35‒3.49, P < 0.01), hyperglycemia (OR 2.01, 95% CI 1.26‒3.22, P < 0.01) during ICU stay, and respiratory diseases (OR 1.9, 95% CI 1.12‒3.23, P = 0.018). Isolation of NRF was independently associated with a lower risk of high-PA (OR 0.43, 95% CI 0.26‒0.73, P < 0.01).
Antibiotic Therapy And Outcomes
VFDs and ICU mortality in patients without VA-LRTI were similar in all groups, with median values of 20‒26 days and 4‒13%, respectively, and were not significantly different in patients receiving AAT or inappropriate antibiotic therapy (IAAT). Association of antibiotic therapy with outcomes in patients with VA-LRTI are shown in Table 4. In patients with VAT, VFDs in low- and moderate-PA groups did not vary significantly with appropriateness for antibiotic therapy. On the other hand, in the high-PA group, VFDs of patients who received IAAT were markedly lower than the VFDs of those who received AAT. Patients with VAP had shorter VFDs, particularly in the moderate- and high-PA groups. ICU mortality tended to be decreased in VAP patients in the low- and moderate-PA groups who received AAT, as compared to those who did not (0‒16.7% vs. 45.5‒46.2%). Patients with high-PA VAP had a very high mortality rate, even with AAT (41.7%). We performed separate propensity score matching for VAT patients within each density group (Table 4, right panel). After matching, although not statistically significant due to the small numbers, AAT was also associated with an improvement in VFDs, but only in the high-PA group (median 0 vs. 17 days, P = 0.06), and not in the low- and moderate-PA groups. Kaplan–Meier analyses among matched patients showed that weaning from MV was almost identical between AAT and IAAT in both the low- and moderate-PA groups, while, in the high-PA group, a lower and later incidence of weaning success were observed with IAAT as compared to with AAT (Fig. 2).
Table 4
Association of antibiotic therapy with outcomes in patients with VA-LRTI
| | Before propensity scores matching | After propensity scores matching |
| | IAAT | AAT | | IAAT | AAT | |
| VFDs at 28 days | n | median (IQR) | N | median (IQR) | P-value | n | median (IQR) | N | median (IQR) | P-value |
| VAT | | | | | | | | | | |
| Low PA | 33 | 24 (0‒27) | 26 | 22 (14‒25) | 0.37 | 22 | 24 (0‒26) | 22 | 23 (12‒25) | 0.85 |
| Moderate PA | 49 | 22 (0‒27) | 47 | 21 (0‒25) | 0.44 | 35 | 23 (0‒27) | 35 | 21 (0‒25) | 0.38 |
| High PA | 33 | 0 (0‒20) | 48 | 19 (0‒24) | 0.02 | 25 | 0 (0‒22) | 25 | 17 (0‒22) | 0.06 |
| VAP | | | | | | | | | | |
| Low PA | 11 | 13 (0‒22) | 5 | 9 (5‒19) | 1 | | | | | |
| Moderate PA | 13 | 0 (0‒19) | 6 | 0 (0‒23) | 0.8 | | | | | |
| High PA | 23 | 0 (0‒0) | 12 | 0 (0‒13) | 0.41 | | | | | |
| ICU mortality | n/N | % | n/N | % | P-value | n/N | % | n/N | % | P-value |
| VAT | | | | | | | | | | |
| Low PA | 1/33 | 3% | 3/26 | 11.5% | 0.2 | 1/22 | 4.6% | 3/22 | 13.6% | 0.61 |
| Moderate PA | 3/49 | 6.1% | 9/47 | 19.2% | 0.054 | 2/35 | 5.7% | 6/35 | 17.1% | 0.26 |
| High PA | 9/33 | 27.3% | 8/48 | 16.7% | 0.25 | 9/25 | 36% | 6/25 | 24% | 0.54 |
| VAP | | | | | | | | | | |
| Low PA | 5/11 | 45.5% | 0/5 | 0 | 0.07 | | | | | |
| Moderate PA | 6/13 | 46.2% | 1/6 | 16.7% | 0.22 | | | | | |
| High PA | 11/23 | 47.8% | 5/12 | 41.7% | 0.73 | | | | | |
| AAT appropriate antibiotic therapy, IAAT inappropriate antibiotic therapy, IQR interquartile range, PA Pseudomonas aeruginosa, VFDs ventilator-free days, VAP ventilator-associated pneumonia, VAT ventilator-associated tracheobronchitis |
{kind=link}
{kind=link}