Study population
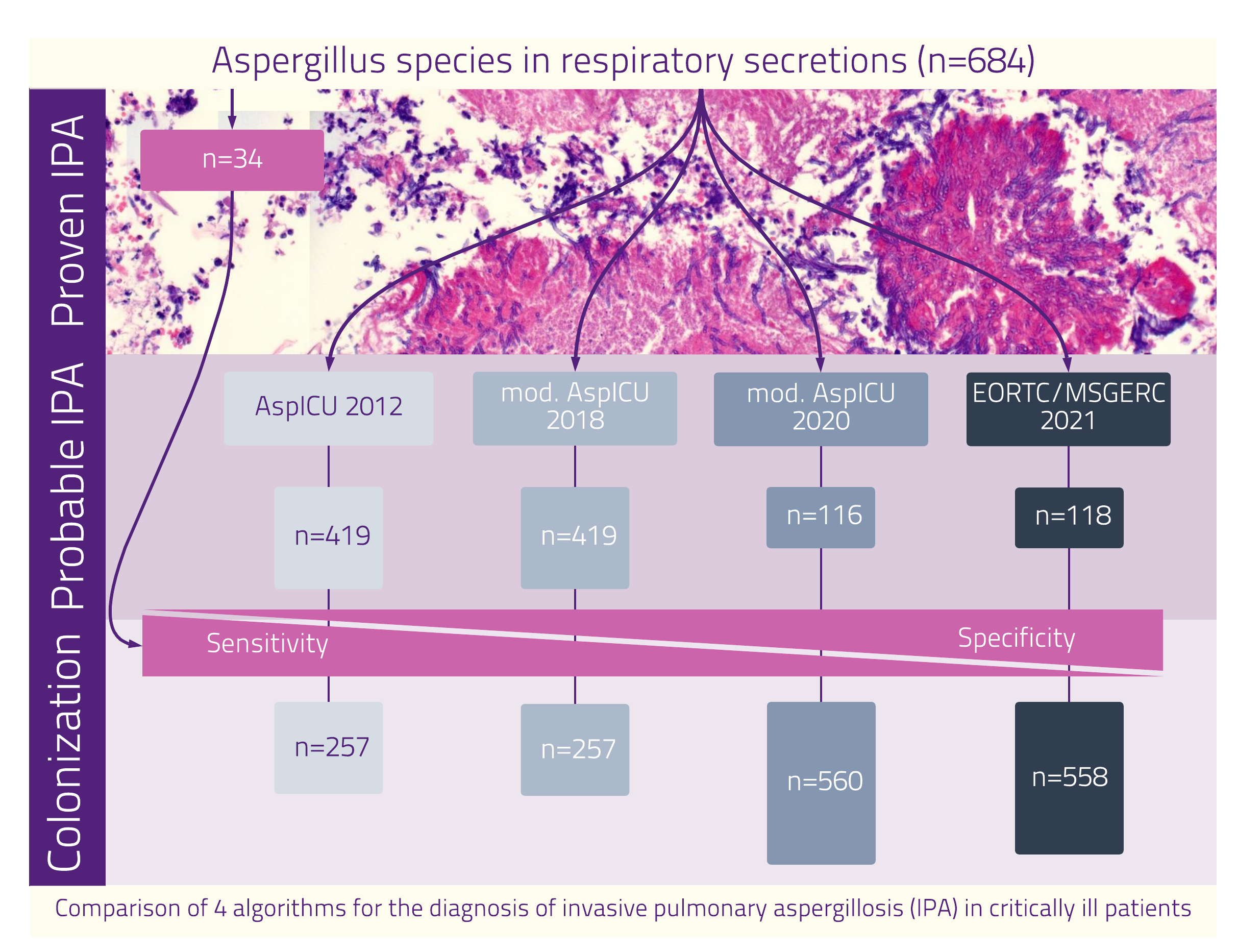
During the study period from 2005 to 2020, we identified 684 patients with a positive Aspergillus culture from respiratory secretions.The flow of participants is shown in Figure 1.The median age was 63 years (IQR 52-73). More than two thirds of patients (n=472, 69%) were admitted to the ICU due to medical conditions with a median length of stay of 18 days (IQR 9-36). The vast majority (n=630, 92%) of all study participants were mechanically ventilated; 77 (11%) required ECMO support. The ICU mortality was 54% (n=369). At 90 daysafter first Aspergillus detection402 patients (59%) deceased (Table 1). Twenty-eight patients (4%) suffered from severe influenza and 13 (2%) were treated for COVID-19.
Table 1
Baseline demographic and clinical characteristics, critical care management, and outcome data from 684 patients with positive culture of Aspergillus spp. in respiratory secretions. Continuous variables are given as median (1st to 3rd quartile), categorical variables are given as n (%).
|
Demographics
|
|
Sex (female)
|
248 (36)
|
|
Age (years)
|
63 (52-73)
|
|
Body mass index (kg*m-2)
|
25 (22-28)
|
|
Baseline characteristics
|
|
Medical admission
|
472 (69)
|
|
Surgical admission
|
212 (31)
|
|
APACHE II
|
21 (16-26)
|
|
SAPS II
|
49 (39-64)
|
|
SOFA
|
11 (8-14)
|
|
ICU Stay
|
|
|
Ventilation
|
|
No mechanical ventilation
|
20 (3)
|
|
NIV
|
34 (5)
|
|
Mechanical ventilation
|
441 (65)
|
|
NIV and MV
|
189 (28)
|
|
ECMO support
|
77 (11)
|
|
Antifungal treatment
|
445 (66)
|
|
Azole (Voriconazole or Isavuconazole)
|
329 (48)
|
|
Echinocandin (Caspofungin or Anidulafungin)
|
168 (25)
|
|
Liposomal Amphotericin B
|
134 (20)
|
|
Change ofantifungal agent
|
163 (24)
|
|
Combination therapy
|
89 (13)
|
|
ICU LOS (days)
|
18 (9-36)
|
|
Outcome
|
|
ICU mortality
|
369 (54)
|
|
28-day mortality
|
329 (49)
|
|
90-day mortality
|
402 (59)
|
APACHE II: Acute Physiology and Chronic Health Evaluation Score, ECMO: Extracorporeal membrane oxygenation, ICU: Intensive Care Unit, LOS: Length of stay, MV: Mechanical ventilation, NIV: Non-invasive ventilation, SAPS II: Simplified Acute Physiology Score II, SOFA: Sequential Organ Failure Assessment Score
Diagnostic agreement for probable IPA
In addition to microbiological, clinical, and radiological findings the AspICU*2012 and EORTC/MSGERC ICU*2021 criteria require host-relatedrisk factors for the definition of probable IPA. The diagnostic findings stratified by the four algorithms are shown in Table 2.
According to the AspICU*2012 criteria[14], 419 (62%) patients had probable (= putative) IPA. A total of 419 (62%) patients fulfilled the criteria for probable IPA according to the modified AspICU*2018 criteria [5](Figure 1).Importantly, probable IPA based on the AspICU*2012 criteria did not apply to the same individuals than probable IPA based on the modified AspICU*2018 algorithm (Figure 2 and 3). The modified AspICU*2020 criteria and the EORTC/MSGERC ICU*2021 criteria for probable IPA were fulfilled by 116 (17%) and 118 (17%) patients, respectively.
The distribution of probable IPA according to single algorithms and the overlap among the four diagnostic criteria is presented in Figure 2. AspICU*2012 classified 24% (n=101/419) of the patients as probable, with no other diagnostic algorithm classifying them as such. In addition, 39% (n=163/419) of the patients classified as probable IPA by the AspICU*2012 criteria also fulfilled the criteria for probable IPA by the modified AspICU*2018 criteria. Fifty-seven (14%) patients had probable IPA according to AspICU*2012, modified AspICU*2018, and modified AspICU*2020. Also 57 patients (14%), but not the same individuals, had probable IPA based on AspICU*2012, modified AspICU*2018, and EORTC/MSGERC ICU*2021.
Table 2
Probable IPA stratified by the number of patients fulfilling the criteria in each of the four diagnostic algorithms. Continuous variables are given as median (1st to 3rd quartile), categorical variables are given as n (%). The relevant criteria for one specific diagnostic algorithm are highlighted in blue.
|
|
AspICU *2012
n=419
|
modified AspICU*2018
n=419
|
modified AspICU*2020
n=116
|
EORTC/MSGERC ICU*2021
n=118
|
|
Microbiology
|
|
Aspergillus species
|
A. fumigatus
|
366 (87)
|
356 (85)
|
101 (87)
|
99 (84)
|
|
A. non fumigatus
|
53 (13)
|
63 (15)
|
15 (13)
|
19 (16)
|
|
Microscopy
|
mycelium
|
25 (6)
|
18 (4)
|
8 (7)
|
10 (8)
|
|
pseudomycelium
|
3 (1)
|
6 (1)
|
2 (2)
|
3 (3)
|
|
negative
|
391 (93)
|
395 (94)
|
106 (91)
|
105 (89)
|
|
Aspergillus GalactomannanBAL
|
negative
|
70 (17)
|
78 (19)
|
21 (18)
|
12 (10)
|
|
positive
|
184 (44)
|
193 (46)
|
57 (49)
|
66 (56)
|
|
not performed
|
165 (39)
|
148 (35)
|
38 (33)
|
40 (34)
|
|
Aspergillus Galactomannan BAL EIA
|
4 (2-4)
|
4 (2-4)
|
4 (3-4)
|
4 (4-4)
|
|
Aspergillus Galactomannan serum
|
negative
|
111 (26)
|
105 (25)
|
24 (21)
|
29 (25)
|
|
positive
|
44 (11)
|
49 (12)
|
19 (16)
|
27 (23)
|
|
not performed
|
264 (63)
|
265 (63)
|
73 (63)
|
62 (53)
|
|
Aspergillus Galactomannan serumEIA
|
2 (1-4)
|
2 (1-4)
|
1 (1-4)
|
3 (1-5)
|
|
Clinical signs
|
|
Dyspnea; respiratoryfailure
|
419 (100)
|
419 (100)
|
116 (100)
|
118 (100)
|
|
Bronchoscopy with Aspergillus specific lesions
|
none
|
343 (82)
|
342 (82)
|
89 (77)
|
64 (54)
|
|
positive
|
36 (9)
|
35 (8)
|
18 (16)
|
48 (41)
|
|
nobronchoscopy
|
40 (10)
|
42 (10)
|
9 (8)
|
6 (5)
|
|
purulent tracheal secretion
|
239 (57)
|
251 (60)
|
98 (84)
|
74 (63)
|
|
pulmonaryhemorrhage
|
71 (17)
|
77 (18)
|
15 (13)
|
16 (14)
|
|
Body temperature (°C)
|
37 (37-38)
|
37 (37-38)
|
38 (37-38)
|
37 (37-38)
|
|
Leukocytes (Mrd/l)
|
12 (7-19)
|
12 (8-19)
|
15 (10-21)
|
12 (6-20)
|
|
Antibacterialtreatment
|
418 (100)
|
418 (100)
|
116 (100)
|
118 (100)
|
|
Radiology
|
|
Computed tomography with Aspergillus specific lesions
|
none
|
215 (51)
|
217 (52)
|
58 (50)
|
20 (17)
|
|
positive
|
74 (18)
|
85 (20)
|
27 (23)
|
83 (70)
|
|
noimaging
|
130 (31)
|
117 (28)
|
31 (27)
|
15 (13)
|
|
Pathological x-ray
|
419 (100)
|
419 (100)
|
116 (100)
|
109 (92)
|
|
Worsening alveolar infiltrates
|
154 (37)
|
200 (48)
|
116 (100)
|
51 (43)
|
|
Opacites in x-ray
|
none
|
0
|
0
|
0
|
9 (8)
|
|
infiltrate
|
117 (28)
|
157 (37)
|
46 (40)
|
34 (29)
|
|
effusion
|
113 (27)
|
0
|
1 (1)
|
13 (11)
|
|
both
|
189 (45)
|
262 (63)
|
69 (59)
|
62 (53)
|
|
Riscfactors
|
|
Host factors (EORTC)
|
218 (52)
|
174 (42)
|
54 (47)
|
71 (60)
|
|
Neutropenia
|
35 (8)
|
32 (8)
|
11 (9)
|
14 (12)
|
|
Immunosuppressivetreatment
|
162 (39)
|
127 (30)
|
39 (34)
|
56 (47)
|
|
Hematologicaldisease
|
79 (19)
|
64 (15)
|
20 (17)
|
26 (22)
|
|
Chemotherapy
|
87 (21)
|
63 (15)
|
16 (14)
|
22 (19)
|
|
Oncological disease
|
103 (25)
|
95 (23)
|
23 (20)
|
23 (19)
|
|
Allogeneicstemcelltransplantation
|
47 (11)
|
38 (9)
|
10 (9)
|
14 (12)
|
|
Autologousstemcelltransplantation
|
6 (1)
|
6 (1)
|
3 (3)
|
5 (4)
|
|
Lung transplantation
|
10 (2)
|
9 (2)
|
1 (1)
|
4 (3)
|
|
Other SOT
|
46 (11)
|
32 (8)
|
7 (6)
|
18 (15)
|
|
COPD
|
75 (18)
|
68 (16)
|
18 (16)
|
18 (15)
|
|
Decompensatedlivercirrhosis
|
56 (13)
|
48(12)
|
14 (12)
|
21 (18)
|
|
Prednisolone or its equivalent more than 20 mg/day
|
351 (84)
|
259 (62)
|
75 (65)
|
93 (79)
|
|
HIV
|
18 (4)
|
17 (4)
|
3 (3)
|
4 (3)
|
|
Severeinfluenza
|
14 (3)
|
27 (6)
|
9 (8)
|
7 (6)
|
|
COVID-19
|
8 (2)
|
13 (3)
|
7 (6)
|
5 (4)
|
|
|
|
Specificity a
|
0.27 (0.15, 0.41)
|
0.29 (0.17, 0.43)
|
0.78 (0.63, 0.88)
|
0.73 (0.59, 0.85)
|
|
Sensitivity a
|
0.82 (0.65, 0.93)
|
0.65 (0.46, 0.80)
|
0.29 (0.15, 0.47)
|
0.59 (0.41, 0.75)
|
BAL: Bronchoalveolar Lavage, COPD: Chronic obstructive pulmonary disease, COVID-19: Corona Virus Disease 2019, EORTC: European Organisation for Research and Treatment of Cancer, EIA: enzyme-linked immunoassay. HIV: human immunodeficiency virus, SOT: Solid Organ Transplantation
a to detect definite IPA confirmed by histopathological results. (95% Confidence Interval)
Criteria that are relevant for the diagnosis with the respective algorithmare highlighted in bold.
Overall, 543 (79%) patients were found to have probable IPA with at least one diagnostic tool. In contrast, only 29 (4%) patients fulfilled the criteria for probable IPA according to all four algorithms(Figure 2).
Diagnostic agreement between the AspICU*2012 and the modified AspICU*2018 criteria was poor with Cohen’s kappa of 0.29 (95% CI: 0.22, 0.37)(Figure 3). Diagnostic agreement was consistently poor among any one of the four different classifications as reflected by low Cohen’s kappa (Figure 3).
Subgroup analysis for histopathological material
Lung tissue for histopathological examination was available in 85 patients (example presented in Figure 4). A subgroup analysis of biopsy materials showed evidence of confirmed IPA in 40% (n=34/85) of these patients. Irrespective of the presence of confirmed IPA, we applied the four algorithms to these 85 patients. The AspICU*2012 reached a sensitivity of 0.27 (95% CI 0.15, 0.41) and a specificity of 0.82 (95% CI 0.65, 0-93), modified AspICU*2018 of 0.29 (95% CI 0.17, 0.43) and 0.65 (95% CI 0.46, 0.80), modified AspICU*2020 of 0.78 (95% CI 0.63, 0.88) and 0.29 (95% CI 0.15, 0.47) and EORTC/MSGERC ICU*2021 of 0.73 (95% CI 0.59, 0,85) and 0.59 (95% CI 0.14, 0.57) respectively (Table 3).
Table 3 Specificity and sensitivity for patients with examination of lung tissue for histopathological examination. (95% Confidence Interval).
|
|
AspICU *2012
n=419
|
modified AspICU*2018
n=419
|
modified AspICU*2020
n=116
|
EORTC/MSGERC ICU*2021
n=118
|
|
Histopathology n= 85
|
Specificity
|
0.27 (0.15, 0.41)
|
0.29 (0.17, 0.43)
|
0.78 (0.63, 0.88)
|
0.73 (0.59, 0.85)
|
|
Sensitivity
|
0.82 (0.65, 0.93)
|
0.65 (0.46, 0.80)
|
0.29 (0.15, 0.47)
|
0.59 (0.41, 0.75)
|
|
Subpopulation analysis
|
|
Histopathology without influenza and covid-19 n=80
|
Specificity
|
0.25 (0.14, 0.40)
|
0.29 (0.17, 0.44)
|
0.77 (0.63, 0.88)
|
0.75 (0.60, 0.86)
|
|
Sensitivity
|
0.84 (0.67, 0.95)
|
0.62 (0.44, 0.79)
|
0.25 (0.11, 0.43)
|
0.56 (0.38, 0.74)
|
|
Histopathology with severe immunosuppression n=48
|
Specificity
|
0.12 (0.03, 0.31)
|
0.28 (0.12, 0.49)
|
0.68 (0.46, 0.85)
|
0.60 (0.39, 0.79)
|
|
Sensitivity
|
0.96 (0.78, 1.00).
|
0.65 (0.43, 0.84)
|
0.30 (0.13, 0.53)
|
0.52 (0.31, 0.73)
|
Subgroup and sensitivity analyses
A subgroup analysis of severely immunocompromised patients (n=256, 37%) (defined as neutropenia, hematological malignancy, chemotherapy, stem cell transplantation, human immunodeficiency virus positivity, solid organ transplantation and/or immunosuppressive medication) revealed very poor agreement among the four diagnostic criteria (Additional File 2). Sensitivity and specificity for immunocompromised patients with lung tissue histopathology (n=48) are presented in Table 3.
To further determine the diagnostic accuracy of the four diagnostic algorithms, we repeated the agreement analyses in a subgroup of patientswithout viral pneumonia (influenza and COVID-19;n=635). Cohen’s kappa again revealed very poor agreement(Additional File 3). In addition, we determined the diagnostic accuracy of confirmed IPA for the subgroup of patients (n=80) with lung tissue excluding patients with viral community-acquired pneumonia (influenza and SARS-CoV-2; Table 3).
{kind=link}