OPSCC incidence is rising at an alarming rate in the United States.2, 3, 15, 16 The most recent analysis completed in 2018 demonstrated a persistently low rate of HPV preventive vaccination among the US population.17 It is, therefore, reasonable to expect that the current increase in OPSCC incidence secondary to HPV is likely to continue for at least the next few decades, especially in North and South America, Central, Eastern, and Northern Europe.18 As the OPSCC patient population is expected to increase, it is critical to improve our understanding of how disease biology interacts with and/or determines treatment response.2, 3, 8, 15, 16 This requires not only an improved understanding of HPV-mediated effects on tumorigenesis and treatment response, but also a better understanding of the interaction between HPV exposure and other OPSCC risk factors such as tobacco exposure.
Despite continued decrease over the last half century, tobacco use remains associated with 4 out of 5 leading causes of death in the US.19 The interplay among smoking, HPV infection, other risk factors, and carcinogenesis is complex and multifactorial.20 Increasing tobacco exposure has been linked to greater hazard of contracting and persisting oral HPV infection in healthy individuals, displaying a prominent dose-response fashion.21–23 The interaction between tobacco exposure and HPV infection in OPSCC carcinogenesis and whether the risk of HPV-mediated OPSCC is higher or lower among smokers have been a matter of ongoing debate.24–26 Our data in the US veteran population indicates that tobacco exposure is nearly ubiquitous and that approximately 75% of new HPV+ OPSCC diagnoses occur in patients with >10 pack-year history of tobacco exposure.8 Similar data have been reported for other patient populations including the indigent, uninsured and underinsured patients.27, 28
The 8th Edition of the AJCC staging manual recognized the more favorable prognosis in patients with HPV-mediated OPSCC. As such, the current staging has downstaged patients with what was historically regarded as locally advanced disease and assigned high stage designation. However, while recognizing that patients with HPV-mediated disease have better prognoses, it has also been recognized that current and former smokers tend to have worse survival rates than non-smokers.7 The AJCC was challenged with incorporating smoking into the staging, which was later described in the manual as follows: “the role of tobacco as a negative prognostic factor is well established. However, exactly how this could be codified in the staging system is less clear”.29 Even prior to the AJCC 8th edition era, similar challenges were reported when smoking was introduced to prognostic framework like in the study by Huang et al. where the model appeared robust for Stages I and II (by criteria used for 8th edition) at a threshold of 20 PY but did not hold in Stage III. That was attributed to the detrimental influence of age in the model, potentially related to inability to tolerate intensive treatment for these anatomically more extensive HPV+ lesions (T4 and N3).30 Our data strongly suggest that, although survival is greatly impacted by HPV status, tobacco exposure also plays a very important role. This has been strikingly demonstrated by a poorer survival in both HPV+ and HPV- heavy smokers (i.e. more than double the hazard of death) compared to <30 PY smokers. This suggests that not all HPV+ OPSCC tumors should be expected to demonstrate the same excellent outcomes we have come to expect. Perhaps most concerning is the significant survival decrease in patients with heavy tobacco exposure. For overall survival, tobacco exposure erases the favorable survival impact of HPV positivity, generating an absolute survival decrement of approximately 16%. As a point of reference, the absolute survival benefit for the addition of chemotherapy to radiation was only ~8%, based on the most recent MACH-NC meta-analysis.31 We recently updated survival for patients with oral cavity SCC, and identified the relative effect size for nodal metastasis at ~15% and extra-nodal extension at ~20%.32 These data place the impact of tobacco exposure within the range of other treatment modifying clinical-pathologic parameters.
Furthermore, our results showed that the impact of heavy tobacco exposure is alarmingly impacting the outcomes of even early stage disease as defined by the newest edition of the AJCC staging system. Our results showed that our proposed tobacco exposure cutoff of 30 py clearly stratified patients at each AJCC (8th edition) stage in terms of overall survival outcomes. However, statistical significance was only reached in stage I, probably because of smaller numbers of patients with more advanced disease, i.e. ~60% of the whole cohort was categorized as stage I. Nonetheless, heavy smokers with stage I or II disease had 5-year outcomes that were approximating or -in some cases- even worse than outcomes of patients with lower smoking index and more advanced disease stage. This observation must be considered in the inclusion criteria for future dose de-escalation studies in early stage HPV+ OPSCC. In agreement with these results, a recent study by Vawda et al.33 has demonstrated that higher intensity of smoking exposure was associated with poorer outcomes in a cohort of exclusively HPV+ oropharyngeal cancer patients treated with primary radiation or surgery. The study, however, lacked the comparison with an HPV- cohort. As a result, the relative effect size of tobacco exposure in the HPV+ OPSCC population remains only partially contextualized. Our findings track closely with those of this recently published data. Moreover, our data indicate that HPV+ patients with smoking index above 30 have surprisingly comparable outcomes to HPV- patients, highlighting the importance of considering this very important risk factor in the treatment decision making process.
In the meantime, the putative impact of smoking on cancer-specific mortality in HPV+ OPSCC subpopulation cannot be interpreted barring the known adverse effects of smoking on general co-morbidity and death, including cardio-vascular, cerebrovascular, pulmonary, other cancers, and co-existing risk factors (e.g. alcoholism), among others.34, 35 Our competing risk analysis indicated that the worse survival outcomes of HPV+ heavy smokers were attributable to two main factors; the increased risk of locoregional failure that leads to more cancer related deaths as well as the overall increased risk of non-cancer related deaths compared with smokers below the identified threshold. (Figures 3 and 4) That’s to say HPV+ heavy smokers who don’t die of smoking-related comorbidities (the dominant detrimental effect of smoking per Figure 3D) will more probably die of loco-regional failure (Figure 4D).
Although large this is a single institution patient cohort and as such our findings must be validated in additional patient cohorts. It is also important to note, that our outcomes for HPV- patients in this series are dramatically better than historical data even from our institution.1, 2, 6 This, combined with the relative small size of the HPV- cohort may confound the comparison between the 3 groups outlined in Figure 1. Moreover, chemotherapy, despite being associated by multiple randomized controlled trials with better treatment outcomes, was not shown to be an independent prognostic factor even in HPV- subpopulation where more benefit from chemotherapy would be expected.36 This can be attributed in part to the retrospective nature of the study where treatment decisions followed the institutional multidisciplinary protocol. That’s to say, patients with early OPC, with more favorable prognosis, received no chemotherapy in contrast to the more advanced HPV-OPC patients who still showed worse outcomes despite receiving chemotherapy.
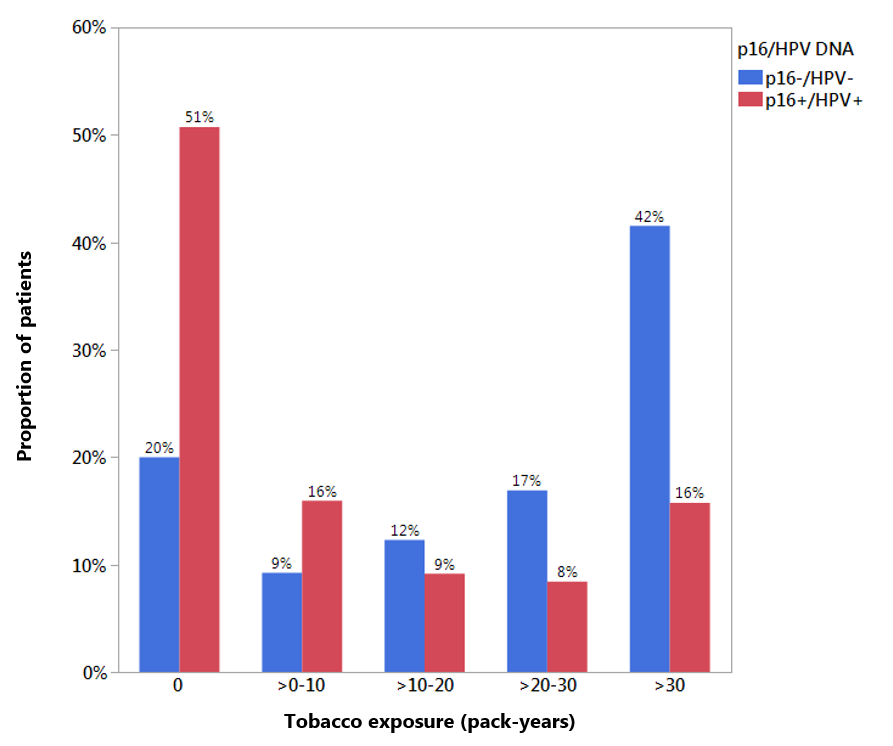
In addition, the tobacco exposure range for the HPV+ cohort is substantially skewed toward the lower range of exposure (Supplementary Figure 2), likely limiting our ability to generate a more granular, dose-dependent effect for tobacco exposure on survival. Moreover, data suggests that current smoking status adversely affects LRC and OS in patients with HNSCC.37, 38 This is further exacerbated by the smoking-induced reduction of radiation-induced tumor killing with subsequent worsening of locoregional control.39, 40 The unavailability of smoking status for patients while on-treatment –as is the case with our study- might raise a question on the weight that should be assigned to the carcinogenic effect of smoking compared to its antagonistic impact on radiotherapy efficacy. Nonetheless, our results showed no differential disease control or overall survival between current and former smokers, even in the heavy smoker subset (PY >30). We acknowledge that our study lacks a detailed categorization of history of tobacco exposure per the International Classification of Diseases, Tenth Revision (ICD–10) diagnosis code, as a result of inherent flaws of retrospective data collection.41 However, it is still intuitive to extricate from our results the useful public health message relating to advice concerning smoking cessation, especially during radiotherapy course.42 Benefits can include limiting radiotherapy/chemotherapy treatment prolongation or interruption and associated heavy symptom burden during and following treatment, in addition to the rapid return of carboxyhemoglobin levels in patients who quit to that of light /never smokers.43, 44
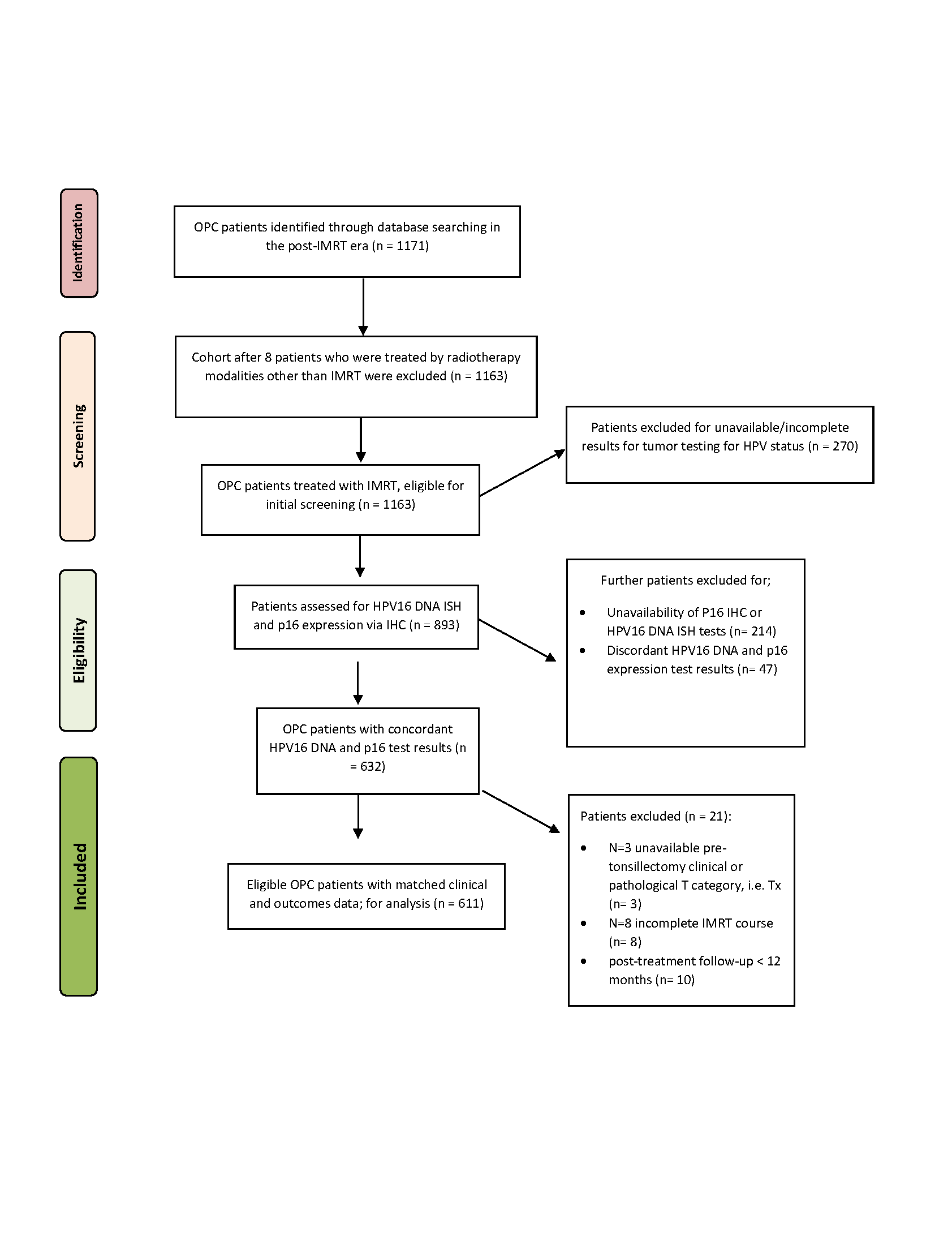
Conversely, by limiting our analysis to only those patients with concordant p16 and HPV testing data, we can feel very confident that however limited the data, it is in fact reflective of the underlying tumor biology and not simply a testing artifact. The data generated here conform to what we have come to expect from OPSCC defined by conventional risk factor exposure (i.e. tobacco exposure), namely decreased treatment response and a high rate of loco-regional failure. We previously showed that >90% of recurrence/progression occurs loco-regionally in a patient cohort with significant tobacco exposure.8 The fact that tobacco exposure is a distinct competing risk for loco-regional failure not only suggests an impact on treatment effectiveness, but is particularly concerning when considering current efforts to de-escalate treatment for HPV+ OPSCC patients.
{kind=link}
{kind=link}