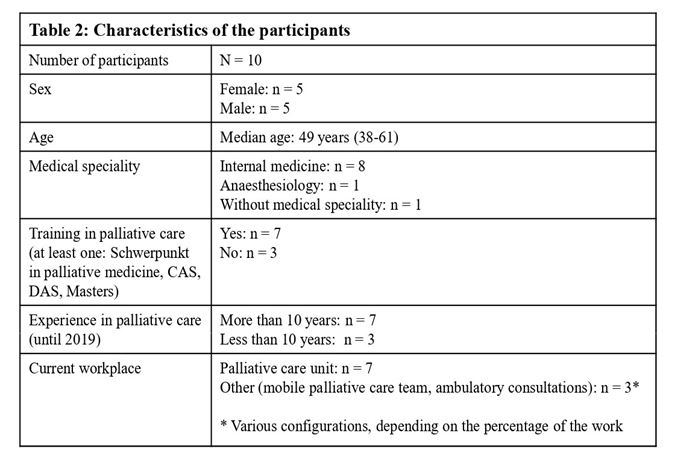
In total, the main researcher contacted nine palliative care structures by email, all of which replied. Six structures agreed to participate in the study: four of them participated and two did not because of the progressive inclusion design and data saturation. The sample size is presented in Fig. 2.
a) Sedation in palliative medicine and assistance in suicide are different approaches
First, it should be clarified that all the physicians (except one) clearly differentiated sedation in palliative medicine from assistance in suicide. They stated that contrary to assistance in suicide, sedation is a palliative treatment based on medical indication.
One physician explained it as follows:
[...] they are two different things: in the first [assisted suicide], the person wants to end his life and in the other [sedation] the person is in a situation where nothing can be done for him, this is unbearable and we decide to induce a therapeutic treatment. So, we are squarely in another thing.
Another physician stated it in this way:
I think they are two completely different approaches: one is a life-sustaining therapeutic approach and the other is killing yourself. And these two different approaches must remain different.
Thus, theoretically, palliative care physicians should never consider sedation as an alternative to assisted suicide. As one physician explained it:
We are not going to propose sedation in place of assisted suicide. [...] I think that the proposal for sedation at the request of assisted suicide is a great drift.
Another physician illustrated it as follows:
“I think that it is not an answer [sedation in place of assisted suicide], it is not A = B. In other words,
it is not that the patient is talking about assisted suicide that we should think about sedation. [...] I don’t think we can say that as soon as the patient talks about assisted suicide, it should be assimilated to sedation because in this context sedation is a form of suicide or an alternative to suicide.”
All participants reported that when a patient requests assistance in suicide, the first step they take is to engage in extended and repeated discussions with him or her, without judging the decision, in order to better understand the reasons for the request. Here is an illustration by one physician:
[...] it is necessary to welcome that [this request], to accompany, to understand what is hidden behind. Often it is desperation, it’s fear, a fear of suffering, a loss of meaning... this feeling of being a burden, this feeling of being useless... then this desire to disappear, this desire for it to be stopped, this need to be freed from a situation that is becoming unbearable.
In all cases, the participants try to improve the holistic care:
We try to take into account the depression, the pain, the financial and psycho-social problems, everything that concerns the whole family, the entourage. We try to do everything.
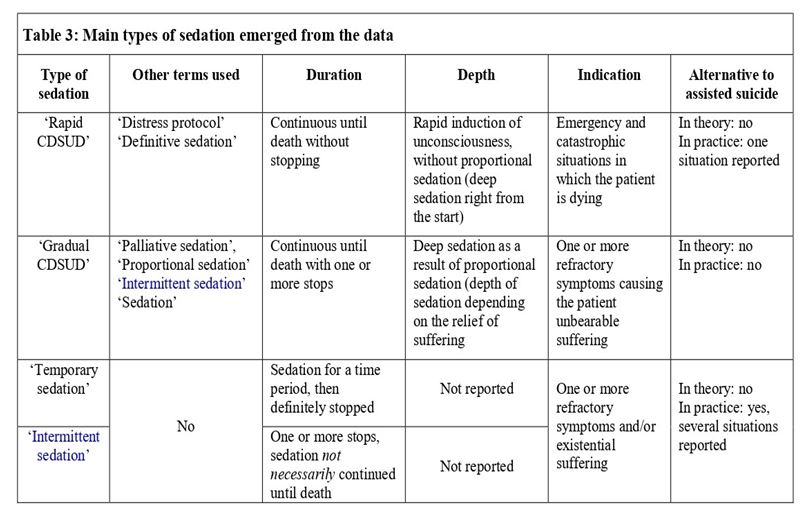
If, despite this, the patient’s wish for assisted suicide persists, most participants re-evaluate the clinical and personal situation. If the request for assisted suicide persists because of unbearable suffering, physicians discuss the possibility of sedation. They clearly stated that sedation should only be introduced for medical reasons, not as an alternative to assisted suicide. However, they reported situations in which sedation, although not medically indicated, was introduced in response to an assisted suicide request. Our linguistic analysis showed four main types of sedation, which we called ‘rapid CDSUD’, ‘gradual CDSUD’, ‘temporary sedation’ and ‘intermittent sedation’. These types of sedation are presented in Table 3.
b) Rapid CDSUD is not considered as an alternative to assisted suicide
Most of the participants stated that sedation to induce unconsciousness rapidly, without proportional sedation (in other words, deep sedation right from the start), and continuously until death without stopping – called ‘definitive sedation’ or a ‘distress protocol’ – is only induced in emergency and catastrophic situations, such as a massive haemorrhage or asphyxia in dying patients. One physician stated:
They are emergency situations, truly irreversible situations for which we think we will have zero potential improvement to hope and in addition we must act quickly. [...] Yes, that is rather in emergency situations, when the patient is choking or bleeding. Similarly, if the patient is epileptic and resistant to all drugs, it doesn’t make much sense to wake him up and he re-convulses.
Another physician reported it as follows:
[…] someone is bleeding out. He is dead in 5 minutes. Continuous deep sedation until death is so required.
Participants pointed out that in all other medical situations, another type of sedation is chosen. As one physician explained:
In principle, when we are not in emergency, we induce sedation just to relieve, so the depth will depend on the relief. We always start with temporary sedation [...]
Another participant added:
The fact of switching to a deep and permanent form of sedation also means straightaway imposing the definitive nature of the loss of contact. This seems difficult to manage in practice (managing with the team, the family, patient himself).
All participants explicitly stated that this type of sedation is never considered as an alternative to assisted suicide.
However, one participant reported a very exceptional situation: although rapid CDSUD was not medically indicated and going home was possible, it was initiated as a response to an assisted suicide request. This sedation lasted several days. The participant described the context:
It was four or five years ago. A patient who was 70 years old [...] was here [in the palliative care unit] for mental distress and for uncontrollable pain in the post-operative period. He wanted to call Exit, then he did the Exit procedures. At the same time, the pain was difficult to relieve, we had to quickly increase the doses. The next day, he was a little drowsy, he was less well and suddenly they (the team) stopped everything and then the pain came back much stronger. This patient was very demanding. Already before, he didn’t want to live [...]; for himself, it was not the quality of life as he imagined. So that was the reason he called Exit. And the pain just added what it took to really want to die. After stopping the analgesic drugs, suddenly, they tried to juggle the analgesia, but never succeeded, and they ended up sedating him. When I came back (I wasn’t there during that time; it was during the weekend), the patient was sedated without any attempt to rehabilitate from the analgesia. He was sedated.
and clearly pointed out the type of sedation:
It was not intermittent sedation in order to see if he could complete the Exit project... He was sedated during two or three weeks, which meant he was physically fine... So, there, I was wondering. For me, it was a kind of ... it was as the title of your study [laughs].
Apart from this one situation reported by a single participant, no similar situation was reported, despite explicit questioning during the interview.
b) Gradual CDSUD is not considered as an alternative to assisted suicide
Most of the participants stated that deep sedation as a result of proportional sedation (depth of sedation depending on the relief of suffering) that was continuous until death with one or more stops – called ‘palliative sedation’, ‘proportional sedation’, ‘intermittent sedation’ or ‘sedation’ – is administered to relieve one or more refractory symptom(s) causing the patient unbearable suffering1. The depth of this sedation always depends on the relief of suffering; it is not deep from the start. One physician explained it as follows:
“There is not only one sedation. Sedation is really patient-focused. It is really done for every patient. There is no comparison. […] There are sedations more or less deep. We have clinical tools (scales) to assess it, such as RASS scales. I never aim, from the start, to have RASS − 3 or -4. My goal is to see if the person feels comfortable […]”
Another physician specified that
It is never immediately deep. In the end, the patient sleeps, it is true.
This sedation is intermittent and, in the last step, continued until death. The participant elucidated:
Until death...It is very common to say: ‘This person, we have already sedated him one night, two nights, three nights’, and then we see that when we wake him up, it is worse. Thus, we say ‘we will continue the sedation and it will be until death’.
Many participants insisted that a proposal of this type of sedation is always based on medical indication; it is not considered as an alternative to assisted suicide. Here are two examples of explanations:
No [palliative sedation cannot be considered as an alternative to assisted suicide]. If an intolerable symptom is the motive for an assisted suicide request, [...] we can offer sedation to relieve this symptom, but only for this objective.
If medical conditions are right, we can always propose palliative sedation, before going home and contacting Exit. In this case, sedation is not an alternative to assisted suicide, because it is induced for medical indications.
However, one physician considered ‘palliative sedation’ as an alternative to assisted suicide in this case. He explained:
You want to know whether sedation is an alternative to Exit. So, purists will always say ‘no, especially not!’, because we must not mix it. I think we must especially not hide our face […]. In fact, it is a form of alternative. People who say that it is not true ... Hm ... In principle, I think we must be honest and have the courage to say: ‘Yes, it is [a form of alternative to assisted suicide], it permits to die by disconnecting from everything that has become unbearable’.
c) Temporary or intermittent sedation is considered as an alternative to assisted suicide
Most of the participants also talked about ‘temporary’ or ‘intermittent’ sedation. Contrary to rapid or gradual CDSUD, these types of sedation are not necessarily continuous until death. They are also administered to relieve one or more refractory symptoms and/or existential suffering, and induced for a time period determined in advance, then definitely stopped (‘temporary sedation’) or continued, sometimes until death (‘intermittent sedation’). The physicians did not say anything about the depth of these forms of sedation. This aspect did not emerge from our data, so it is not known if this sedation is proportional or deep from the start.
Participants pointed out that these types of sedation are administered in response to appropriate medical indication(s) and cannot be considered as an alternative to assisted suicide. However, most participants reported situations in which these forms of sedation, although not medically indicated, were introduced in response to an assisted suicide request. This was especially due to the impossibility of carrying out an assisted suicide at home (e.g., due to home transfer not being possible or the patient’s wish not to traumatize the family). Three physicians explained:
[...] it happens. I’ve seen it. There are a lot of reasons why patients don’t carry out assisted suicide: ‘I don’t want to come back home, because my husband/wife and my children are there. And then, after that they will live in the house where I committed suicide’. It is very difficult. Other reasons: ‘My family doesn’t want me to do Exit because it’s against their values, because they don’t want it to traumatize them. So, I am looking for an alternative’. There are patients who are bedridden, they are not independent, they are hospitalized and then, they say: ‘I can’t go back home. Kill myself, yes, I want to do it. But I can’t go back home. Physically, it’s impossible for me’. [...] So, there are many reasons which make that (it comes from the patient himself or his family) that finally the option ‘assisted suicide’ is aborted. [...] As assisted suicide can’t be carried out, we naturally look for an alternative...
[...] on the one hand, yes, that’s a kind of alternative. I have already seen patients in the unit who would like assisted suicide and for various reasons it was not possible, and we say OK and finally we induced sedation. In this context, sedation is a kind of alternative to assisted suicide. These situations are not very common.
There are patients whose wish was clear. They were a member of Exit all their life, they are determined, they want to realize an assisted suicide but, unfortunately, the evolution of their disease has meant that they can’t go back home, they can’t swallow anymore, they are not conscious enough to swallow. Just because it’s too late doesn’t mean they don’t have the right to be relieved. So, there, in this context, sedation is [...] an alternative to assisted suicide [...]
Finally, one participant reported a specific and highly exceptional situation: intermittent sedation was administered as an alternative to assisted suicide because of the impossibility of the patient returning home; however, this sedation proved to be ineffective and the only possible solution was to perform an assisted suicide in the palliative care unit as an exceptional case. He explained:
[...] the ultimate argument was: the impossibility of going home. She said: ‘we refuse to realize an assisted suicide in our house that we built, that we wanted, which was the object of our dreams... We refuse to leave that to our children as an inheritance’. She refused to do this at home and she said that for her it was ethically impossible. And it is true that we had no arguments to go against our own arguments. [...] This situation is very interesting because we proposed intermittent sedation to this patient. And then she said OK, why not. [...] But it went very badly. The dose was increased. Despite this, she woke up. The awakening was catastrophic. She felt very badly. [...] Assisted suicide was exceptionally realized here, in this palliative care unit.
Footnote:
[1] Conceptualizations of ‘refractory symptoms’ and ‘suffering’ are not presented in this paper.
{kind=link}
{kind=link}