There is increasing evidence that the current mechanism of IVIG in the treatment of KD mainly involves the immune response, the destruction and remodelling of the blood vessels and endothelial inflammation, including regulating the activation of T cells and other antigen-presenting cells; regulating Fc receptor expression and inhibiting complement activation; regulating the production of cytokines and inhibiting immune response; neutralizing bacterial super antigens and toxins; and so on [21-23]. Based on these perspectives, it is hypothesized that laboratory markers of inflammation and endothelial function parameters would be reliable predictors. There have been numerous studies [24-26] about the predictive value of laboratory markers for IVIG resistance in KD, but few reports have examined endothelial function parameters and the correlation between these two main indicator types.
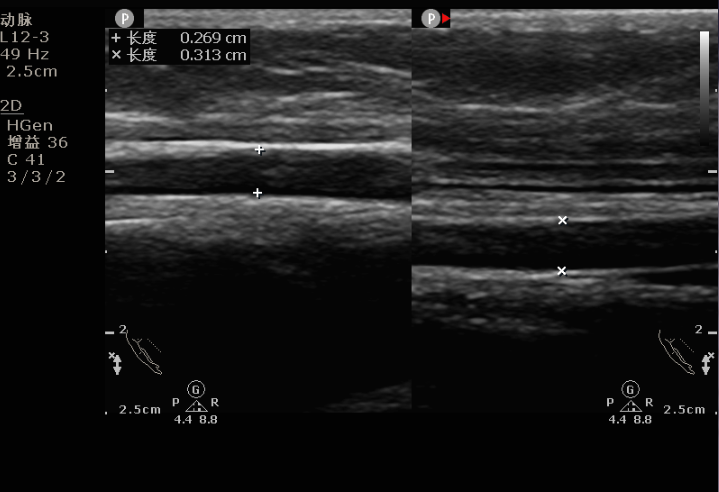
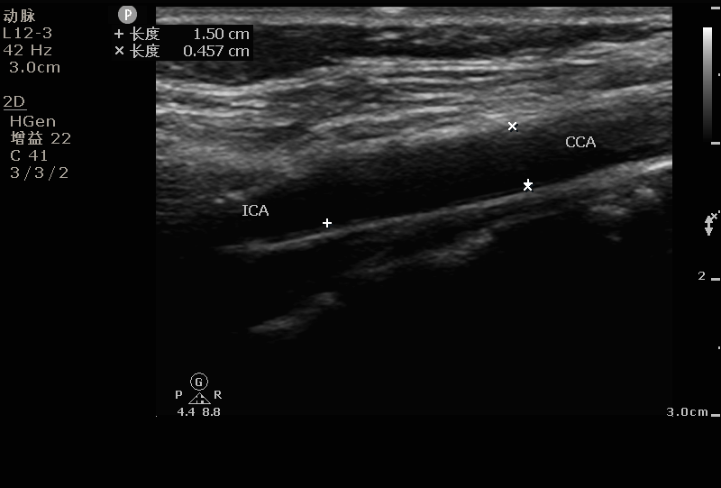
In our investigation, we demonstrated that IVIG-resistant KD patients had both significantly lower FMD and higher CIMT than other groups, despite the differences in SI in these groups not reaching statistical significance. However, we did not find any difference in endothelial parameters between AURI patients and normal children. These findings confirmed that common infection-related febrile factors may not be sufficient to cause either obvious swelling of the vascular medial membrane or serious damage to the structure of the arterial wall and that simple and transient inflammation in the acute phase may not be sufficient to cause significant premature arteriosclerosis in a short time [27]. In addition, there was lower FMD and higher CIMT in IVIG-resistant patients than in the IVIG-sensitive patients, which means that endothelial dysfunction in IVIG-resistant KD patients may be more serious than that in IVIG-sensitive patients and AURI patients. There was no significant difference in CIMT between the IVIG-sensitive and AURI groups. Therefore, FMD may be more reliable in KD children for the assessment of endothelial function in the acute phase than CIMT and SI. In further logistic analysis, we found that of the three vascular ultrasonography parameters, only FMD (< 5.79%) was an independent predictor of IVIG resistance, which also confirmed the above hypothesis. FMD was created as a high-frequency ultrasound technique for a surrogate marker of endothelial vasodilation function by Celermajer et al [16] in 1992. It works by physically blocking the brachial artery, resulting in transient ischaemia and hypoxia, which stimulates the endothelium to release nitric oxide and other associated vasodilators (neurohormones such as acetylcholine, 5-hydroxytryptamine and catecholamine). When the physical blockage is removed, vessels with normal endothelial function expand in response to a large number of these cytokines and molecules [28]. Compared with SI and CIMT, which focus on evaluating vascular morphology [29], FMD mainly monitors vasodilation function after artificial mechanical stimulation physiologically [16, 30]. Since endothelial cell activation and dysfunction are earlier observable changes than structure and form in the development of vascular diseases in lesion areas[31] and measurement of FMD includes online monitoring of disturbed blood flow dynamics, FMD can more sensitively reflect the difference between the vascular endothelium of patients with IVIG resistance and other groups under the influence of systemic inflammation. In adults, FMD<5 indicates impaired endothelial function, but there is no established standard in children [32]. In the present study, the cut-off value predicted by FMD for IVIG resistance was lower than the normal range but significantly lower than that of the healthy control group. Therefore, it was speculated that most IVIG-resistant KD patients had subclinical endothelial dysfunction, as the correlation between them may be undesirable consequences of inflammatory storms.
In the analysis of laboratory markers of inflammation in KD patients, similar to the distinctly different vascular ultrasonography parameters between the IVIG-sensitive and IVIG-resistant groups mentioned above, there were statistically significant differences in NT-proBNP, which reflects myocardial ischaemia and hypoxia; Na+, which mainly reflects microvascular permeability and interleukin levels; and inflammatory parameters, such as N%, PCT and ALB, which also support the release and cascade reaction of systemic inflammatory factors and vasculitis in IVIG-resistant patients, which were stronger and more inadequate for remission, consistent with some results of previous studies[24-26]. Among those laboratory data, aggressive inflammatory response (PCT>1.69 ng/ml) and hyponatremia (Na+<133.2 mmol/L) were found to be strong independent predictors of IVIG resistance in KD children, similar to FMD (<5.79%), through multivariate logistic regression analysis. Only PCT had a larger AUC than FMD, which had the highest sensitivity with a value of 78.0%, indicating that FMD could be a better predictor than most of the laboratory data above. PCT is an acute-phase reactant whose levels are not affected by the administration of corticosteroids or nonsteroidal anti-inflammatory medication. As a prohormone for calcitonin, it is suppressed or nonresponsive to interferon-γ, moderately responsive to tumour necrosis factor-α (TNF-α) and interleukin-6 (IL-6) stimulation, and strongly responsive to interleukin-1β (IL-1β) [26]. Previous studies reported that increased IL-6 and IL-1β may activate ADH secretion and aggravate microvascular permeability in KD patients with severe inflammation, leading to SIADH and hyponatremia[25]. This process partially has the same inflammatory mediators as PCT, which means that PCT is partly correlated with microvascular permeability. Both hyponatremia and elevated PCT are closely related to excessive expression of inflammatory factors.
In the context of immune-mediated injury, the vascular endothelium may trigger a low-level inflammatory response by imitating pathogen- and damage-associated molecular patterns and activating monocyte-derived macrophages, T cells, B cells, dendritic cells and mast cells by affecting substrate-receptor interactions and the secretion of different mediators[30] in inflammation, coagulation, angiogenesis and tumour invasion. In our follow-up correlation analysis, the negative correlations between FMD and PCT in both the KD group and subgroups were stronger in the IR group than in the IS group, while hyponatremia was not significantly correlated with FMD since a possibly larger part of FMD involves endocrine and neuroregulatory mechanisms[25] rather than endothelial inflammation. These findings further confirmed that a severe exaggerated inflammatory response can lead to vascular damage through biochemical and immune damage pathways[30] and is an important mechanism of vascular structure and endothelial function damage in IVIG-resistant patients[33, 34]. At the same time, there may be considerable overlap between inflammatory responses that lead to elevated PCT and pathophysiological processes (including injury of endothelial cells that release vasodilators and blocking of vasodilator response pathways in the vascular wall that influence vasodilation) in IVIG-resistant patients. This may be related to cytokines such as TNF-α, IL-6, and IL-1β[30]. Even though FMD<5.79% (OR=3.563) has a good predictive ability for IR, PCT>1.69 ng/ml had a higher OR (4.257), which means that abnormally elevated PCT has a stronger directivity to IR than FMD. Therefore, we speculate that changes in the morphology and function of vessel walls lag behind inflammation in KD[35], which is also believed to be the initial step in many other rheumatic diseases, including systemic lupus erythematosus, ankylosing spondylitis, Bechet’s disease, rheumatoid arthritis, and so on[36].
Although further basic experimental proof is needed, the above conclusions might provide a clue for future aetiologic studies on IVIG resistance in KD. Additionally, we suggest that before IVIG treatment, if either FMD, PCT or Na is found to be abnormally different from their critical values, we recommend the timely strengthening of endothelial nutritional support, extra anti-inflammatory therapy such as hormone application, regulation of water and electrolyte homeostasis and other measures that can promote the control of inflammation to a certain extent to prevent the occurrence of IVIG resistance. Similarly, in children with drug resistance to IVIG, strengthening the above measures is likely to prevent the recurrence of drug resistance and refractory KD [3, 23, 37, 38]. While the combination of FMD and PCT as a diagnostic tool in routine clinical practice is not yet warranted, in the absence of reliable tools for diagnosing IVIG-resistant KD, this investigation could prove useful in the future.
Our study has several limitations. First, the sample size of this study was small, and all subjects in this study were Chinese. Further large-scale, multicentre prospective studies are needed to confirm our findings. Second, to acquire ultrasonic data, we measured only the right neck for CIMT and SI and only the left brachial artery for FMD, while LVEF and LVFS were measured only in the KD group, which may have led to some selection bias. Third, the laboratory data were limited in our study; we did not collect laboratory data for the AURI and normal groups, and thus, more indicators need to be included prospectively.
{kind=link}
{kind=link}
{kind=link}
{kind=link}