Background: the hyperinflammation phase of severe SARS-CoV-2 is characterized by complete blood count alterations. In this context, the neutrophil to lymphocyte ratio (NLR) and the platelet to lymphocyte ratio (PLR) can be used as prognostic factors. We study NLR and PLR trends at different timepoints and compute optimal cutoffs to predict four outcomes: use of Continuous Positive Airways Pressure (CPAP), ICU admission, invasive ventilation and death.
Methods: we retrospectively included all adult patients with SARS-CoV-2 pneumonia admitted from 23rd January 2020 to 18th May 2021. Data were extracted using ICD9 codes and our Covid-19 registry. Analyses included descriptive statistics and non parametric tests to study the ability of NLR and PLR to distinguish the patients’ outcomes at each timepoint. ROC curves were built for NLR and PLR at each timepoint (minus discharge) in order to identify cutoffs to distinguish severe and non severe disease and their statistical significance was assessed with the Chi-square test. NLR and PLR were compared with DeLong’s test.
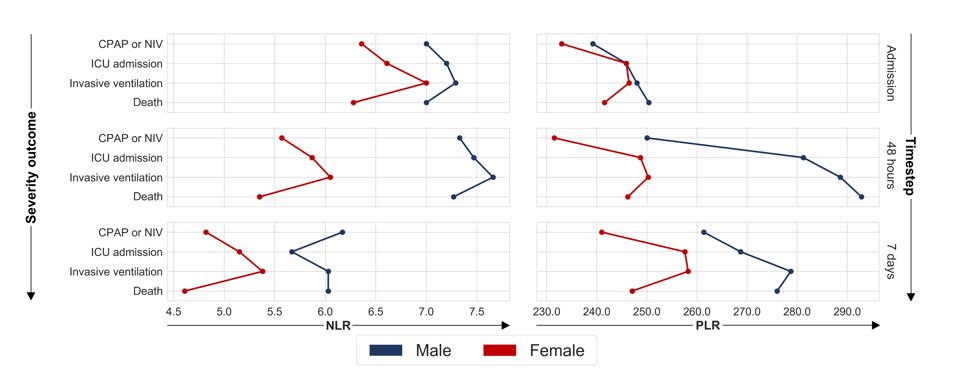
Results: we included 2169 patients. NLR and PLR were higher in severe Covid-19 at all the timepoints, with a difference that gets bigger and a trend that is steeper in more severe disease. Both ratios were able to distinguish the outcomes at each timepoint. For NLR, the areas under the curve (AUROC) ranged between 0.59 and 0.81, for PLR, between 0.53 and 0.67. From each ROC curve we computed an optimal cutoff value (e.g. NLR 7 for CPAP for males at admission). NLR performed better than PLR.
Conclusion: our results are in line with other studies that computed NLR and PLR trends and values in disease, especially with those that distinguished between different grades of severity.
Our study is retrospective and single centre, and is limited by selection bias, but includes more than 2000 patients, thus limiting the confounding factors and outliers.
Our cutoffs do not only deal with severity and mortality but allow for a more tailored approach. Future prospect include validating our cutoffs in a prospective cohort and comparing their performance against other Covid19 scores.
{kind=link}