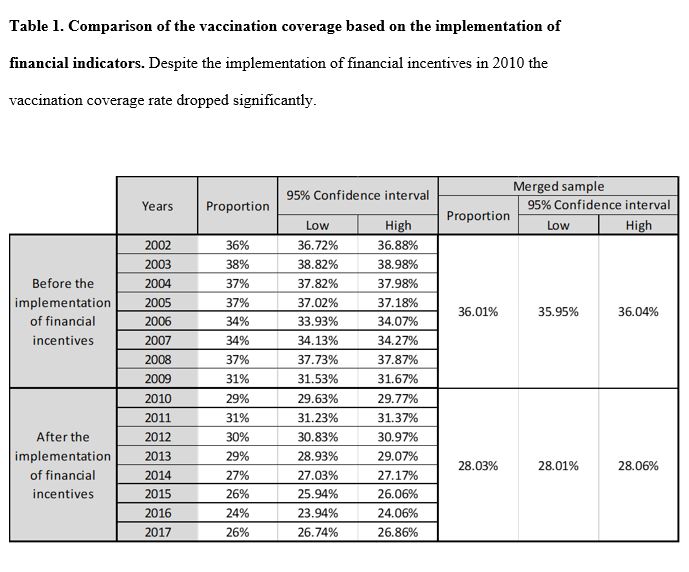
The influenza vaccination coverage is still insufficient despite the introduction of the financial incentive related primary care indicators in Hungary. Although there is a financial motivation for the family physicians to vaccinate their elderly patients against influenza, the flu vaccination coverage is declining in recent years.
However, the results should be interpreted with caution due to several factors which were not investigated this current study (e.g. individual behavioral factors, attitude towards the family physicians). According to the literature there are several factors which might influence the vaccination. A study in 1989 found that older people desire interventions that prolong their lives. Over 65, influenza vaccination is one such intervention. A study of people living in an elderly home found that it was mostly relatives who agreed to such interventions (including interviewing health care providers). The elderly people are often in need of guardianship because of the growing cognitive decline and other health burdens. In the case of patients under guardianship, it may be that the care of the elderly is nowadays solved by professional guardians and it is not the family member who makes the decision in their best interest anymore. It is also important to educate the elderly in a way that is understandable to them so that they can give their informed consent (eg. using vignette with simple language) (15).
According to a study of Mayo AM and Cobler S. in 2004, the best motivating factors for accepting a vaccine were that it had been received previously by the person (93%) and that it was recommended by a health care professional (62%). Besides, the biggest barriers were the fear of side effects (35%) and fear of catching the flu (30%). The basic idea would be that patients perceive themselves to be at high risk and will therefore do more for their health. But even though patients may know what it means to be high risk, they do not consider themselves to fall into this category. It was found that the vaccinated and non vaccinated people had significant differences regarding to four major categories: age, whether they classified themselves as high-risk patients, the number of years of education, and self-rated health. Vaccinated people were older, more likely to be classified themselves as high-risk patients, have higher educational level, and they considered their health worse (16).
An American study found similar results: older people (> 85) and those who had at least high school graduates were more likely to accept the vaccine. The White population was also more likely to receive the vaccine than the Hispanic or African Americans population. Smokers were less likely to receive the vaccination, while those who reported not having seen by a doctor in the past year were 28% less vaccinated, than those who had seen a doctor within one year. When people who did not ask the vaccine was asked why they did not, the distribution of responses was as follows: 20% said they were afraid of side effects or that the vaccine could cause disease, 17% thought that vaccination would not stop the flu or did not know they needed it, 13% thought the vaccine itself could cause the flu. Only 5% said they did not ask because they were not recommended by their doctor to do so and 1% did not ask because of its price (17).
Furthermore, an Italian study found that older people, those who spent less time in education and less healthy patients were more likely to be vaccinated. The latter group includes people with chronic illnesses who have declared themselves to be in poor health. They also found that higher household income and smoking reduced the likelihood of someone being vaccinated (18).
In the US, in the 2018–2019 season, 68.1% of those over 65 were vaccinated (19). According to the ECDC report, 19 of the EU / EEA Member States have reported coverage data of older age groups in recent years. None of these countries achieved the target coverage of 75%. While in the previous study 5 countries were unable to report vaccine coverage, this was 11 in the latest survey. Coverage has declined or stagnated in several countries (20).
There is a significant number of sites on the Internet that are against vaccination. The phenomenon known as Web 2.0 has become ubiquitous and means that interactive and user-generated content is shared. At the same time, a new paradigm was emerging that placed power in the hands of patients instead of the doctors, questioning the legitimacy of science. Together, they have created an environment in which anti-vaccine movements can effectively communicate their messages. People often turn to the Internet for advice on vaccination, which greatly influences them in their decision-making. There have been frequent claims on the Internet that the vaccine causes illness; ineffective; parts of a governmental / health / pharmaceutical conspiracy; the main pharmaceutical trend is incorrect and corrupt (21). The impact of this movement is illustrated by an online survey conducted during a flu pandemic in Canada, showing that 23.4% of people thought the vaccine was safe, 41.4% considered it unsafe and 35.2% were ambivalent about its safety (22). Looking further into this area, during H1N1 influenza in 2009–2010, there was a great deal of fear of vaccines due to the promotion of anti-vaccine activists. In the US, 70 million doses were destroyed, although there was no evidence that the vaccines did harm (23).
{kind=link}