In this study, the role of social cognitive theory constructs as predictive factors of behavior related to the control and prevention of nosocomial infections in hospital nursing staff was evaluated. Structural equation analysis shows that the theoretical model is suitable for the data and explains the nosocomial infections control behavior in the hospital nursing staff. In the test of goodness-of-fit of the final modified model, the absolute fit indices (χ2, and RMSEA), the comparative fit indices (IFI and CFI) and parsimonious fit indices (PCFI and PNFI) met the criteria, indicating that the model-fit well with the data. The literature described that a good model is with insignificant χ2 (p ≥ 0.05), IFI ≥ 0.90, PGFI ≥ 0.50, RMSEA ≤ 0.08, PNFI ≥ 0.50, and CFI ≥ 0.90 (21-23) .
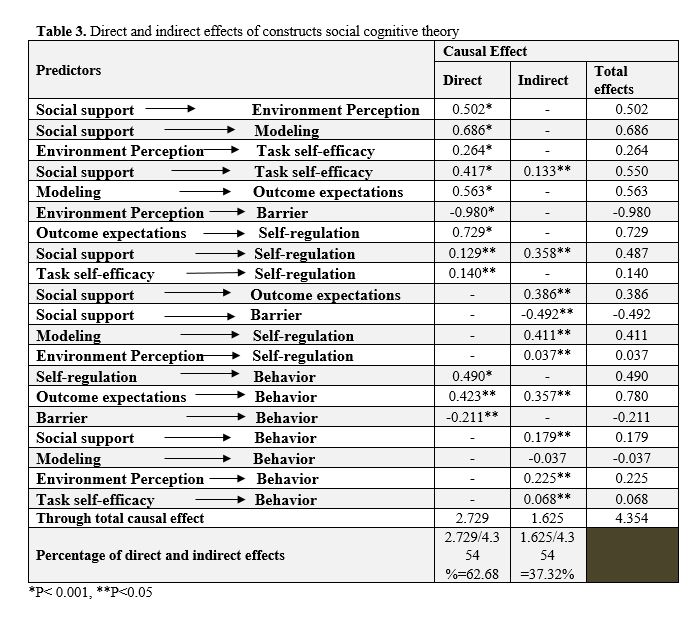
Our research results show that self-regulation directly plays an important role in the performance of hospital nursing in controlling and preventing nosocomial infections. Consistent with these results, a study showed that the process of self-regulatory is an important predictor of hand hygiene (24). In fact, when individuals control their performance, they are more likely to set more realistic and challenging goals, thereby helping to overcome behavioral barriers (25).
In this study, the results show that independent of self-regulatory behaviors, self-efficacy has little effect on behaviors. Consistent with our results, studies have shown that one of the determinants of healthy behavior is self-efficacy, which can predict various healthy behaviors, including prevention of nosocomial infections and hand hygiene (26, 27). Although self-efficacy is often a powerful predictor of behavioral adoption and maintenance in healthy behaviors, a meta-analysis showed that self-efficacy has different effects on healthy behaviors are (28). Researchers also describe people who have a high level of self-efficacy trying harder to achieve their goals when faced with obstacles (29).
In the present study, outcome expectation is influenced by modeling, and directly and indirectly affects the behavior of nursing staff through self-regulation. Other researchers have also shown that observational learning can enhance outcome expectations and can influence behavior (30). Contrary to these results, in another study that showed the results of predicting the constructs of protection motivation theory integrated with the outcome expectation construct of the social cognitive theory related to protective measures against Ebola infection, the outcome expectation construct did not predict the protective behaviors of nurses against Ebola infection (31).
The results of this study indicate that the perceived environment affects barriers. Barriers also have a direct and negative effect on the preventive behavior of nosocomial infections in hospital nurses. Consistent with these results, other studies have shown that barriers such as insufficient knowledge, personal attitude and judgment, environmental constraints, and insufficient leadership skills have a negative effect on nurses' adherence to standard precautions (32-35).
In this study, social support is another determinant of nosocomial infections prevention behavior, which indirectly affects it. The influence of social support on preventive behaviors of nosocomial infections was through self-regulation, self-efficacy, perceived environment and modeling. Based on these results, the literature describes that self-efficacy and social support are important facilitator of self-regulation, especially planning (36). In another studies, social support, including institutional and management support for stablishing a safe environment and providing facilities, had a significant impact on compliance with standard precautions (such as hand hygiene)(37-39).
Our results showed that modeling has a negative effect on the preventive behavior of nosocomial infections in hospital nursing staff. This factor also had an indirect effect on behavior through barriers. The literature points out that the role of a mentors as a role model affects the hand hygiene behavior of nursing students (40). In another study, the lack of appropriate role models was identified as one of the problems of non-compliance with standard perceptive measures, which was caused by environmental factors and barriers (including conflicts between professional, unsupported organizational culture and financial issues (41).
In the present study, perceived environment had an indirect effect on the preventive behavior of nosocomial infections in the hospital nursing staff through barriers. Consistent with these results, earlier studies have shown that environment factors (for example, lake of access to personal protective equipment, heavy workload, and crowded ward) can have a significant impact on compliance with standard precautions by healthcare staff (42, 43).
Limitations
This study tested the predictive effect of social cognitive theory constructs on a set of behaviors preventing nosocomial infections. While, previous studies have examined factors related to hand hygiene behavior. This study was conducted in all intensive care units in several hospitals, therefore, the generalized findings are appropriate. One of the weaknesses of the study is that the effect of knowledge and demographic factors such as age, gender and education, which have been identified in previous studies as important factors on adherence to preventive behaviors of nosocomial infections, was not examined. This study was also conducted in teaching hospitals that have special conditions in the hospitalization, treatment and nursing-care processes, and therefore it is necessary to examine the interaction of environmental, personal and behavioral factors in other non-teaching and private hospitals.
{kind=link}