Thirty quantitative, observational studies (35 papers) met the inclusion criteria. The total number of students that participated in the quantitative studies was 17,013, with studies ranging in size from 57 to 3706. Eighteen studies recruited student participants from only one university; five studies 29–38 included seven or more universities. Six studies 36–42 only recruited first year students, while the majority of studies recruited students from a range of year groups. Five studies 40, 43–46 recruited only, or mainly, psychology students which may impact on the generalisability of findings. A number of studies focused on students studying particular subjects including: nursing 47 medicine 48, business 49, sports science 50. One study 51 recruited LGBTQ students, and one 52 recruited students who had attended hospital having self-harmed. In 27 of the studies, there were more female than male participants. The mean age of the participants ranged from 19.1 to 28 years. Ethnicity was not reported in 19 of the studies. Where ethnicity was reported, the proportion that were ‘white British’ ranged from 71–90.4%. See Table 1 for a summary of the characteristics of the included studies and the participants.
Table 1
Table of included studies
|
Author (year)
|
Design
|
Participants
|
Universities
|
Year group
|
subjects
|
% female
|
% BAME
|
Mean age
|
|
Berry (2012)43
|
CS -QS
|
57
|
1
|
3.5% (n = 2) 1st year
75.4% (n = 43) 2nd year
1.8% (n = 1) 3rd year
19.3% (n = 11) postgraduate
|
72% psychology
|
86%
|
NR
|
21.2
|
|
Boulton (2019)53
|
Longitudinal QS
|
175
|
1
|
49% 1st year
49% 1st year
27% 2nd year
21% 3rd year
|
multiple
|
66%
|
NR
|
NR
|
|
Davies (2019)54
|
longitudinal /prospective
|
325
|
NR
|
NR
|
NR
|
70.8%
|
NR
|
NR
|
|
Denovan (2017a)44
|
longitudinal 1 year
|
192
|
1
|
NR
|
psychology
|
82%
|
|
19,7
|
|
Denovan (2017b)64
|
CS QS
|
202
|
1
|
NR
|
social science students
|
73.8%
|
NR
|
22.8
|
|
El Ansari (5 papers) (2013, 2014 a,b,c 2015)29–32, 74
|
CS QS
|
3706
|
7
|
NR
|
NR
|
72.8%
|
|
24.9
|
|
Freeth(2012)63
|
CS QS
|
1325
|
1
|
NR
|
NR
|
61.90%
|
|
20.1
|
|
Gorczynski (2017)
|
CS QS
|
330
|
1
|
54.4% 1st year
|
NR
|
44.2%
|
NR
|
20.9
|
|
Gnan(2019)34
|
CS QS
|
1948
|
multiple
|
NR
|
NR
|
46.9%
|
NR
|
20.3
|
|
Hassel (2018)45
|
CS QS
|
77
|
1
|
NR
|
psychology
|
80.5%
|
|
19.1
|
|
Hixenbaugh (2012)39
|
CS QS
|
429
|
1
|
1st year
|
NR
|
69% F
|
|
21.8
|
|
Holliman (2018)40
|
Longitudinal survey
|
186
|
1
|
1st year
|
psychology
|
75%
|
76% from UK
'most' were white British
|
19.2
|
|
Honney (2010)48
|
CS QS
|
853
|
1
|
NR
|
medicine (n = 553) non-medical (n = 300)
|
66%
|
37.4%
|
?
|
|
Jackson (2015)35
|
CS QS
|
230
|
multiple
|
NR
|
NR
|
52%
|
NR
|
21.3
|
|
Jessop (2020)70
|
CS QS
|
337
|
1
|
1st year students, 101 (29.97%) 2nd year, 117 (34.72%) 3rd year
and 24 (7.12%) fourth year.
|
NR
|
69.1%
|
|
21.1
|
|
Kotera (2019)49
|
CS QS
|
138
|
1
|
NR
|
business
|
49%
|
29% international students
|
21.2
|
|
Lloyd (2014)62
|
CS QS
|
315
|
3
|
NR
|
NR
|
83%
|
92% UK born
95% spoke English as their primary language at home
|
23.4
|
|
Mahadevan (2010)52
|
case control
|
261
|
1
|
NR
|
NR
|
70%
|
|
?
|
|
McIntyre (2018)56
|
CS QS
|
1135
|
1
|
• 1st -year students comprised 46%
• 2nd - and 3rd year students made up 35% and 21%, respectively.
|
• Health and Life Sciences (30%), Humanities and Social sciences (42%) and Science and Engineering (18%)
|
71%
|
82% white
|
20.8
|
|
McLafferty (2019)41
|
CS QS
|
739
|
4
|
1st year
|
NR
|
61%
|
|
21
|
|
Nightingale (2013)42
|
longitudinal (1 year)
|
331
|
1
|
1st year
|
multiple
|
53.6%
|
White British 87.2%
|
18–49
|
|
Norbury (2019)46
|
CS QS
|
546
|
2
|
1st 291 (53)
2nd 225 (41)
3rd 30 (6)
|
89% psychology
|
84%
|
N R
|
20.4
|
|
Oliver (2010)50
|
CS QS
|
146
|
1
|
1st or 2nd year
|
sports science
|
33.6%
|
|
19.3
|
|
O'Neill (2018)51
|
longitudinal retrospective (1year)
|
739
|
1
|
NR
|
NR
|
62.5%
|
NR
|
21
|
|
Por (2011)47
|
prospective correlational survey
|
130
|
NR
|
range
|
nursing
|
90%
|
47.7% British
18.5% African
4% Asian
4% Caribbean
|
28
|
|
Richardson (2017a,2017b,2018)37, 55, 57
|
longitudinal survey (12–14 months)
|
454
|
1
|
range
|
NR
|
77.9 %
|
89.6% white
|
19.9
|
|
Richardson (2015)36
|
Longitudinal
|
390
|
every university
|
1st year
|
multiple
|
77.9%
|
90.4% White British
|
19.8
|
|
Taylor (2020)60
|
CS QS
|
707
|
2
|
NR
|
multiple faculties
|
75.2%
|
83.0% White
|
23.1
|
|
Thomas (2020)67
|
CS QS
|
510
|
multiple
|
1st year
|
multiple
|
60.8%
|
49.6 British
|
18–24 (n = 476)
|
|
Tyson (2010)68
|
CS QS
|
100
|
1
|
NR
|
NR
|
80%
|
|
20.4
|
| NR: Not reported, CS QS: Cross-sectional Questionnaire, Survey |
Table 1: Table of included studies
Design and quality appraisal of the included studies
The majority of included studies (n = 22) were cross-sectional surveys. Nine studies (in 10 publications) 36, 37, 40, 42, 44, 51–55 were longitudinal in design, recording survey data at different time points to explore changes in the variables being measured. The duration of time that these studies covered ranged from 19 weeks to 12 years. Most of the studies (n = 18) only recruited participants from a single university. In most of the studies, students were invited to participate, in three questionnaires were sent to all students. The methods of recruitment, the use of one university setting and the large number of studies that recruited only psychology students weakens the wider applicability of the included studies.
Quantitative Variables
Included studies (n = 30) measured a wide range of variables and explored their association with poor mental health and wellbeing. These included individual level factors: age, gender, sexual orientation, ethnicity and a range of psychological variables. They also included factors that related to mental health variables (family history, personal history and mental health literacy), pre-university factors (childhood trauma and parenting behaviour. University level factors including social isolation, adjustment and engagement with learning. Their association was measured against different measures of positive mental health and poor mental health.
Measurement of association and the strength of that association has some limitations in addressing our research question. It cannot prove causality, and nor can it capture fully the complexity of the inter-relationship and compounding aspect of the variables. For example, the stress of adjustment may be manageable, until it is combined with feeling isolated and out of place. Measurement itself may also be misleading, only capturing what is measureable, and may miss variables that are important but not known. We included both qualitative and PPI input to identify missed but important variables.
The wide range of variables and different outcomes, with few studies measuring the same variable and outcomes, prevented meta-analyses of findings which are therefore described narratively.
The variables described were categorised during the analyses into the following categories:
Vulnerabilities – factors that are associated with poor mental health
Individual level factors including; age, ethnicity, gender and a range of psychological variables were all measured against different mental health outcomes including depression, anxiety, paranoia, and suicidal behaviour, self-harm, coping and emotional intelligence.
Age
Seven studies41, 43, 47, 48, 51, 56, 57 examined a student’s ages and association with mental health. There was inconsistency in the study findings, with studies finding that age (21 or older) was associated with fewer depressive symptoms, lower likelihood of suicide ideation and attempt, self-harm, and positively associated with better coping skills and mental wellbeing. This finding was not however consistent across studies and the association was weak. Theoretical models that seek to explain this mechanism have suggested that older age groups may cope better due to emotion-regulation strategies improving with age58
Sexual orientation
Four studies34, 41, 59, 60 examined the association between poor mental health and sexual orientation status. In all of the studies LGBTQ students were at significantly greater risk of mental health problems including depression41, anxiety41, suicidal behaviour34, 41, 60, self harm34, 41, 60, use of mental health services34 and low levels of wellbeing59. The risk of MH problems in these students compared with heterosexual students, ranged from OR 1.4 to 4.5. This elevated risk may reflect the greater levels of isolation and discrimination commonly experienced by minority groups.
Gender
Nine studies34, 39–41, 43, 48, 51, 56, 57 examined whether gender was associated mental health variables. Two studies34, 48 found that being female was statistically significantly associated with use of mental health services, having a current mental health problem, suicide risk, self harm34 and depression48. The results were not consistent, with another study56 finding the association was not significant. Three studies40, 41, 43 that considered mediating variables such as adaptability and coping found no difference or very weak associations
Ethnicity
Two studies48, 56 examined the extent to which ethnicity was associated with mental health One study48 reported that the risks of depression were significantly greater for those who categorised themselves as non-white (OR 8.36 p = 0.004). There was no significant difference in the McIntyre et al (2018) study56. The small number of participants from ethnic minority groups represented across the studies means that this data is very limited.
Family factors
Six studies34, 41, 43, 51, 56 explored the association of a concept that related to a student’s experiences in childhood and before going to university. Three studies41, 51, 56 explored the impact of ACEs (Adverse Childhood Experiences) assessed using the same scale by Feletti (2009)61 and another explored the impact of abuse in childhood47. Two studies examined the impact of attachment anxiety and avoidance43, and parental acceptance62. The studies measured different mental health outcomes including; positive and negative affect, coping, suicide risk, suicide attempt, current mental health problem, use of mental health services, psychological adjustment, depression and anxiety.
The three studies that explored the impact of childhood trauma (ACE’s) all found a significant and positive relationship with poor mental health amongst university students. O’Neill et al (2018) in a longitudinal study (n = 739) showed that there was in increased likelihood in self-harm and suicidal behaviours in those with either moderate or high levels of childhood adversities (OR:5.5 to 8.6)51. McIntyre et al (2018)56 (n = 1135) also explored the impact of childhood trauma through multiple regression analysis with other predictive variables. They also found that childhood trauma is significantly positively correlated with anxiety, depression and paranoia (ß =0.18, 0.09, 0.18) though the association is not as strong as the correlation seen for loneliness (ß=0.40)56. McLafferty et al (2019)41 explored the compounding impact of childhood adversity and negative parenting practices (over-control, overprotection and overindulgence) on poor mental health (depression OR 1.8, anxiety OR 2.1 suicidal behaviour OR 2.3, self-harm OR 2.0).
Gaan et al’s (2019) survey of LGBTQ students (n = 1567) found in a multivariate analyses that sexual abuse, other abuse from violence from someone close, and being female had the highest odds ratios for poor mental health and were significantly associated with all poor mental health outcomes34.
While childhood trauma and past abuse poses a risk to mental health for all young people it may place additional stresses for students at university. Entry to university represents life stage where there is potential exposure to new and additional stressors, and the possibility that these students may become more isolated and find it more difficult to develop a sense of belonging. Students may be separated for the first time from protective friendships. However, the mechanisms that link childhood adversities and negative psychopathology, self-harm and suicidal behaviour are not clear 41. McLafferty et al (2019) also measured the ability to cope and these are not always impacted by childhood adversities41. They suggest that some children learn to cope and build resilience that may be beneficial.
McLafferty et al (2019)51 also studied parenting practices. Parental over-control and over-indulgence was also related to significantly poorer coping (OR -0.075 p < 0.05) and this was related to developing poorer coping scores (OR -0.21 p < 0.001)41. These parenting factors only became risk factors when stress levels were high for students at university. It should be noted that these studies used self-report, and responses regarding views of parenting may be subjective and open to interpretation. Lloyd et al’s (2014) survey found significant positive correlations between perceived parental acceptance and students’ psychological adjustment, with paternal acceptance being the stronger predictor of adjustment.
Autism
Autistic students may display social communication and interaction deficits that can have negative emotional impacts. This may be particularly true during young adulthood, a period of increased social demands and expectations. Two studies35, 63 found that those with autism had a low but statistically significant association with poor social problem-solving skills and depression.
Mental Health History
Three studies48, 52, 59 investigated mental health variables and their impact on mental health of students in higher education. These included; a family history of mental illness and a personal history of mental illness.
Students with a family history or a personal history of mental illness appear to have a significantly greater risk of developing problems with mental health at university48. Mahadevan et al (2010)36 found that university students who self-harm have a significantly greater risk (OR 5.33) of having an eating disorder than a comparison group of young adults who self-harm but are not students.
Buffers – factors that are protective of mental wellbeing
Psychological factors
Twelve studies30, 35, 40–44, 47, 50, 60, 64, 65 assessed the association of a range of psychological variables and different aspects of mental wellbeing and poor mental health. We categorised these into the following two categories: firstly, psychological variables measuring an individual’s response to change and stressors including adaptability, resilience, grit and emotional regulation40–44, 47, 50, 62, 64, 65 and secondly, those that measure self-esteem and body image30, 60
The evidence from the eight included quantitative studies suggests that students with psychological strengths including; optimism, self-efficacy44, 64, 66, resilience, grit65, use of positive reappraisal50, having better coping behaviours43 and emotional intelligence47,42 are more likely to experience greater mental wellbeing (see Table 2 for a description of the psychological variables measured). The positive association between these psychological strengths and mental well-being had a positive affect range from r = 0.2–0.5 and OR1.2742, 44, 47, 50, 64, low to moderate strength of association. The negative associations with depressive symptoms are also statistically significant but with weaker association (r=-0.2—0.3)44, 50, 64.
Denovan (2017a)34 in a longitudinal study found that the association between psychological strengths and positive mental wellbeing was not static and that not all the strengths remained statistically significant over time. The only factors that remained significant during the transition period were self-efficacy and optimism, remaining statistically significant as they started university and 6 months later
Table 2
Summary of psychological variables evaluated in the included studies
|
Variable
|
Definition
|
|
Academic self-efficacy
|
• a belief in one’s ability to achieve desired results from one’s behaviour in academic settings Students high in academic self-efficacy perceive tasks, difficulties, and setbacks as challenges to be overcome rather than threats.
|
|
Adaptability
|
• the extent to which an individual is able to adjust and modify (manage) cognitive (thoughts), behavioural (actions) and emotional (affective) functioning in the face of changing, novel and uncertain circumstances, situations or conditions
|
|
Body image
|
• the mental image we have of the size, shape and contour of our own bodies as well as of our feelings about these characteristics and the parts that constitute our bodies
|
|
Coping
|
• Strategies adopted to reduce stressors. These can include problem focused approaches or emotion focused strategies and individuals may adopt a variety during the course of a stressful situation
|
|
Emotion regulation
|
• how a person control expresses, and manages their emotions which plays a very important role in how they cope and respond to stress.
|
|
Emotional Intelligence
|
• type of social intelligence that involves a person's ability to monitor their own and others' emotions, to discriminate among them and to use that information to guide their thinking and actions.
|
|
Grit
|
• working strenuously towards challenged, maintaining effort and interest over years despite failure, adversity, and plateaus in progress.”
|
|
Hope
|
• an individual’s perceived capability to develop a pathway to achieve a goal assumes future outcomes are influenced by goal-oriented cognitions
|
|
Optimism
|
• a generalised positive outcome expectancy, positive expectations that good outcomes will happen, perceive these outcomes as attainable, and persevere in goal-oriented efforts
|
|
Positive psychology
|
• a theoretical approach that focusses on positive individual traits, valued subjective experiences, and positive institutions. it emphasises an understanding of the processes and factors that contribute to the health, success, and flourishing of individuals..
|
|
Resilience
|
• the ability to recover from adversity and react adaptively to stressful situations and is a core component of psychological well-being
|
|
Self esteem
|
• the extent to which a person accepts, likes, or is satisfied with themselves
|
|
Self-control
|
• the ability to exercise restraint over behaviour to meet long-term interests.
|
|
Self-talk
|
• an intra-personal event that could be interpreted as informational or controlling and may attenuate or exacerbate the negative effects of a stressful experience.
|
Parental factors
Only one study62 explored family factors associated with the development of psychological strengths that would equip young people as they managed the challenges and stressors encountered during the transition to higher education. Lloyd et al (2014)62 found that perceived maternal and paternal acceptance made significant and unique contributions to students’ psychological adjustment. Their research methods are limited by their reliance on retrospective measures and self-report measures of variables, and these results could be influenced by recall bias.
Self image
Two studies30, 60 considered the impact of how individuals view themselves on poor mental health. One study considered the impact of self-esteem and the association with non-accidental self-injury (NSSI) and suicide attempt amongst 734 University students. As rates of suicide and NSSI are higher amongst LGBT students, the prevalence of low self-esteem was compared. There was a low but statistically significant association between low self-esteem and NSSI, though not for suicide attempt. A large survey, including participants from seven universities43 compared depressive symptoms in students with marked body image concerns, reporting that the risk of depressive symptoms was greater (OR 2.93) than for those with lower levels of body image concerns
Mental health literacy and help seeking behaviour
Two studies49, 59 investigated attitudes to mental illness, mental health literacy and help seeking for mental health problems
University students who lack sufficient mental health literacy skills to be able to recognise problems or where there are attitudes that foster shame at admitting to having mental health problems can result in students not recognising problems and/or failing to seek professional help.49, 59 Gorcyznski et al (2017)70 found that women and those who had a history of previous mental health problems exhibited significantly higher levels of mental health literacy. Greater mental health literacy was associated with an increased likelihood that individuals would seek help for mental health problems. They found that many students find it hard to identify symptoms of mental health problems and that 42.3% of students are unaware of where to access available resources. Of those who expressed an intention to seek help for mental health problems, most expressed a preference for online resources, and seeking help from family and friends, rather than medical professionals such as GPs.
Kotera et al (2019)57 identified self-compassion as an explanatory variable, reducing social comparison, promoting self-acceptance and recognition that discomfort is an inevitable human experience. The study found a strong, significant correlation between self-compassion and mental health symptoms (r= -0.6. p < 0.01).
There again appears to be a cycle of reinforcement, where poor mental health symptoms are felt to be a source of shame and become hidden, help is not sought, and further isolation ensues, leading to further deterioration in mental health. Factors that can interrupt the cycle are self-compassion, leading to more readiness to seek help (see Fig. 2).
Figure 2: Poor mental health – cycles of reinforcement
Social Networks
Nine studies 34, 39, 42, 47, 52, 56, 60, 64, 67 examined the concepts of loneliness and social support and its association with mental health in university students. One study also included students at Higher Education Institutions47. Eight of the studies were surveys, and one was a retrospective case control study to examine the differences between university students and age-matched young people (non-university students) who attended hospital following deliberate self-harm52.
Included studies demonstrated considerable variation in how they measured the concepts of social isolation, loneliness, social support and a sense of belonging. There were also differences in the types of outcomes measured to assess mental wellbeing and poor mental health. Grouping the studies within a broad category of ‘social factors’ therefore represents a limitation of this review given that different aspects of the phenomena may have been being measured. The tools used to measure these variables also differed. Only one scale (The UCLA loneliness scale) was used across multiple studies 42, 56, 67. Diverse mental health outcomes were measured across the studies including positive affect, flourishing, self-harm, suicide risk, depression, anxiety and paranoia.
Three studies42, 55, 56 measuring loneliness, two longitudinally42, 55, found a consistently positive association between loneliness and poor mental health in university students. Greater loneliness was linked to greater anxiety, stress, depression, poor general mental health, paranoia, alcohol abuse and eating disorder problems. The strength of the correlations ranged from 0-3-0.4 and were all statistically significant (see Table 3). Loneliness was the strongest overall predictor of mental distress, of those measured.. A strong identification with university friendship groups was most protective against distress relative to other social identities56. Whether poor mental health is the cause, or the result of loneliness was explored further in the studies. The results suggest that for general mental health, stress, depression and anxiety, loneliness induces or exacerbates symptoms of poor mental health over time55, 56. The feedback cycle is evident, with loneliness leading to poor mental health which leads to withdrawal from social contacts and further exacerbation of loneliness.
Factors associated with protecting against loneliness by fostering supportive friendships and promoting mental wellbeing were also identified. Beliefs about the value of ‘leisure coping’, and attributes of resilience and emotional intelligence had a moderate, positive and significant association with developing mental wellbeing and were explored in three studies47, 64, 68.
The transition to and first year at university represent critical times when friendships are developed. Thomas et al (2020)49 explored the factors that predict loneliness in the first year of university. A sense of community and higher levels of ‘social capital’ were significantly associated with lower levels of loneliness. ‘Social capital’ scales measure the development of emotionally supportive friendships and the ability to adjust to the disruption of old friendships as students transition to university. Students able to form close relationships within their first year at university are less likely to experience loneliness (r-0.09, r-0.36, r-0.34). One study39 investigating the relationship between student experience and being the first in the family to attend university found that these students had lower ratings for peer group interactions.
Young adults at university and in higher education are facing multiple adjustments. Their ability to cope with these is influenced by many factors. Supportive friendships and a sense of belonging are factors that strengthen coping. Nightingale et al (2012) undertook a longitudinal study to explore what factors were associated with university adjustment in a sample of first year students (n = 331).42 They found that higher skills of emotion management and emotional self-efficacy were predictive of stable adjustment. These students also reported the lowest levels of loneliness and depression. This group had the skills to recognise their emotions and cope with stressors and were confident to access support. Students with poor emotion management and low levels of emotional self-efficacy may benefit from intervention to support the development of adaptive coping strategies and seeking support.
The positive and negative feedback loops
The relationship between the variables described appeared to work in positive and negative feedback loops with high levels of social capital easing the formation of a social network which acts as a critical buffer to stressors (see Fig. 3). Social networks and support give further strengthening and reinforcement, stimulating positive affect, engagement and flourishing. These, in turn, widen and deepen social networks for support and enhance a sense of wellbeing. Conversely young people who enter the transition to university/higher education with less social capital are less likely to identify with and locate a social network; isolation may follow, along with loneliness, anxiety, further withdrawal from contact with social networks and learning, and depression.
Figure 3: The positive and negative feedback loops
Triggers – factors that may act in combination with other factors to lead to poor mental health
Stress
Stress is seen as playing a key role in the development of poor mental health for students in higher education. Theoretical models and empirical studies have suggested that increases in stress are associated with decreases in student mental health13, 44. Students at university experience the well-recognised stressors associated with academic study such as exams and course work. However, perhaps less well recognised are the processes of transition, requiring adapting to a new social and academic environment (Fisher 1994 cited by Denovan 2017a)44. Por et al (2011)55 in a small (n = 130 prospective survey found a statistically significant correlation between higher levels of emotional intelligence and lower levels of perceived stress (r = 0.40). Higher perceived stress was also associated with negative affect in two studies44, 47, and strongly negatively associated with positive affect (correlation − 0.62)64.
University variables
Eleven studies36, 40, 48, 52, 53, 56, 57, 64, 67, 69, 70 explored university variables, and their association with mental health outcomes. The range of factors and their impact on mental health variables is limited, and there is little overlap. Knowledge gaps are shown by factors highlighted by our PPI group as potentially important but not identified in the literature (see Box 1). It should be noted that these may reflect the focus of our review, and our exclusion of intervention studies which may evaluate university factors. Box 1 also gives an example of interventions that may have been developed and introduced within universities.
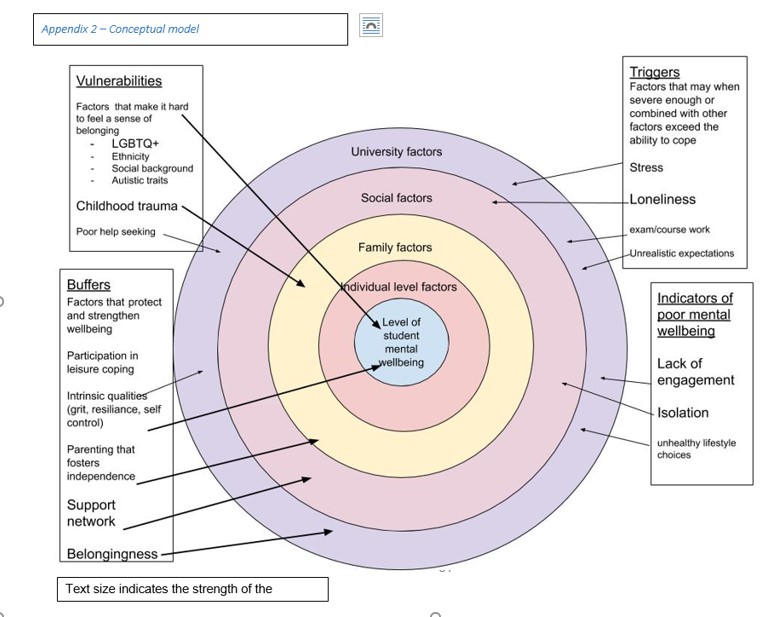
High levels of perceived stress caused by exam and course work pressure was positively associated with poor mental health and lack of wellbeing 52, 53, 64. Other potential stressors including financial anxieties and accommodation factors appeared to be less consistently associated with mental health outcomes36, 39, 48, 52, 55, 56. Important mediators and buffers to these stressors are coping strategies and supportive networks (see conceptual model Appendix 2). One impact of financial pressures was that students who worked longer hours had less interaction with their peers, limiting the opportunities for these students to benefit from the protective effects of social support.
Box 1 Variables highlighted by the PPI group
-
Low morale for BAME groups - ‘all the cleaners were black and the lecturers were white’
-
Lack of of help with learning basic skills like - how to write essays access research
-
Some teaching models make it difficult to integrate
-
Loss of support
-
Have to take responsibility for your own health
-
Peer pressure to say ‘it’s amazing’
-
Health and wellbeing services are hard to see, hard to access or unhelpful
-
Competitive toxic environments
Red flags – behaviours associated with poor mental health and/or wellbeing
Engagement with learning and leisure activities
Engagement with learning activities was strongly and positively associated with characteristics of adaptability40 and also happiness and wellbeing53 (see Fig. 4). Boulton et al (2019)32 undertook a longitudinal survey of undergraduate students at a campus-based university. They found that engagement and wellbeing varied during the term but were strongly correlated. Engagement occurred in a wide range of activities and behaviours. The authors suggest that the strong correlation between all forms of engagement with learning has possible instrumental value for the design of systems to monitor student engagement. Monitoring engagement might be used to identify changes in the behaviour of individuals to assist tutors in providing support and pastoral care. Students also were found to benefit from good induction activities provided by the university. Greater induction satisfaction was positively and strongly associated with a sense of community at university and with lower levels of loneliness67.
These variables are inter-related; greater adaptability is strongly associated with more positive engagement in learning and university life and more engagement is associated with higher mental wellbeing.
Denovan et al (2017b)59 explored leisure coping, its psychosocial functions and its relationship with mental wellbeing. An individual’s beliefs about the benefits of leisure activities to manage stress, facilitate the development of companionship and enhance mood were positively associated with flourishing and were negatively associated with perceived stress. Resilience was also measured. Resilience was strongly and positively associated with leisure coping beliefs and with indicators of mental wellbeing. The authors conclude that resilient individuals are more likely to use constructive means of coping (such as leisure coping) to proactively cultivate positive emotions which counteract the experience of stress and promote wellbeing. Leisure coping is predictive of positive affect which provides a strategy to reduce stress and sustain coping. The belief that friendships acquired through leisure provide social support is an example of leisure coping belief. Strong emotionally attached friendships that develop through participation in shared leisure pursuits are predictive of higher levels of well-being. Friendship bonds formed with fellow students at university are particularly important for maintaining mental health, and opportunities need to be developed and supported to ensure that meaningful social connections are made.
The ‘broaden-and-build theory’ (Fredickson 200471 cited by64) may offer an explanation for the association seen between resilience, leisure coping and psychological wellbeing. The theory is based upon the role that positive and negative emotions have in shaping human adaptation. Positive emotions broaden thinking, enabling the individual to consider a range of ways of dealing with and adapting to their environment. Conversely, negative emotions narrow thinking and limit options for adapting. The former facilitates flourishing, facilitating future wellbeing. Resilient individuals are more likely to use constructive means of coping which generate positive emotion (Tugade & Fredrickson 200472, cited by64). Positive emotions therefore lead to growth in coping resources, leading to greater well-being.
Figure 4: Engagement and wellbeing
Health behaviours at university
Seven studies30, 32, 39, 46, 52, 64, 68 examined how lifestyle behaviours might be linked with mental health outcomes. The studies looked at leisure activities64, 68, diet30, alcohol use30, 32, 39, 52 and sleep46.
Depressive symptoms were independently associated with problem drinking and possible alcohol dependence for both genders but were not associated with frequency of drinking and heavy episodic drinking. Students with higher levels of depressive symptoms reported significantly more problem drinking and possible alcohol dependence32. Mahadevan et al (2010)36 compared students and non-students seen in hospital for self-harm and found no difference in harmful use of alcohol and illicit drugs.
Poor sleep quality and increased consumption of unhealthy foods were also positively associated with depressive symptoms and perceived stress30. The correlation with dietary behaviours and poor mental health outcomes was low, but also confirmed by the negative correlation between less perceived stress and depressive symptoms and consumption of a healthier diet.
Physical activity and participation in leisure pursuits were both strongly correlated with mental wellbeing (r = 0.4)64, and negatively correlated with depressive symptoms and anxiety (r=-0.6, -0.7)68.
{kind=link}