Systematic review
This systematic review was registered with PROSPERO, the International Prospective Register of Systematic Reviews (registration number CRD42019157309) and carried out in accordance with the guidelines for Preferred Reporting Items for Systematic Reviews and Meta-analysis Protocols (PRISMA- P)[25]. All published studies of interest were identified through a search involving the following electronic databases: MEDLINE, PUBMED, EMBASE, CINAHL.
A pre-defined search strategy was formulated which included a combination of relevant medical subject headings (MeSH), associated synonyms and free text [26]. To identify studies reporting a family history the following terms were used; "family" OR "familial" OR "hereditary" OR "heritability" OR "hereditability" OR "inherit" OR "inherited" OR "genetic" OR "genes" OR "gene". These were added to terms for Cluster Headache including "Trigeminal Autonomic Cephalalgia” OR "TACS" OR "Cluster Headache" OR "cluster headaches" combined using the ‘AND’ operator. To ensure a robust review, references from cited articles were also screened. Finally, experts were also consulted to identify additional missed literature. The details of the search strategy used for individual databases is summarised in table 1.
Eligibility criteria and data extraction.
All studies reporting the prevalence of familial cluster headache within a defined cohort of CH patients were included in the analysis. The inclusion criteria defined a positive family history as a clinical diagnosis of CH, in one or more affected individuals, who were a first or second-degree relative. To avoid an over representation of familial history, only studies that confirmed a diagnosis of CH in an affected relative were included in the systematic review. All abstracts were independently analysed by two authors and those fulfilling the eligibility criteria were included for full-text review. A separate assessment of the included studies was conducted by two authors independently and the following data was extracted for analysis: study design, year of publication, population studied, methodology of data acquisition, diagnostic criteria employed, number of participants, gender ratio, percentage reporting a family history and gender ratio of patients with familial CH (Table 2).
To exclude the risk of bias, all eligible studies were independently analysed using a modified Newcastle – Ottawa appraisal checklist, a tool designed to appraise cohort studies on three main areas: the selection of the study groups, the comparability of these groups; and the ascertainment outcome for [27]. The total score of the modified version is limited to 7 stars with removal of sections pertaining only to longitudinal studies (Table 3). All seven studies scored 6 or higher in our risk of bias assessment, demonstrating a low risk of bias, therefore all seven studies were included for meta-analysis
Unpublished cohort
We included an additional unpublished cohort of patients who attended the headache clinic at the National Hospital for Neurology and Neurosurgery (Queen Square, London, UK) between January 2007 and April 2017. All consecutive patients diagnosed with CH, in accordance with ICHD3b, and met our inclusion criteria were recruited with informed consent and underwent a detailed family history as part of their clinical assessment. A diagnosis of cluster headache was confirmed in family members either in clinic or using a semi-structured phone interview based on the ICHD3b criteria. In cases where relatives were uncontactable or deceased, only those with a diagnosis of CH confirmed by a neurologist were deemed eligible. . A total of 645 patients were included in the study. Of these, 456 (70.69%) were male. A family history of cluster headache was reported in 66 patients (10.2%).18 cases were excluded as relatives did not fulfil the ICHD3b criteria for cluster headache or were uncontactable. Overall, 48 (7.44%) individuals had a confirmed family history of CH.
Statistical analysis
Estimation of relative proportion of effected probands with positive family history of CH:
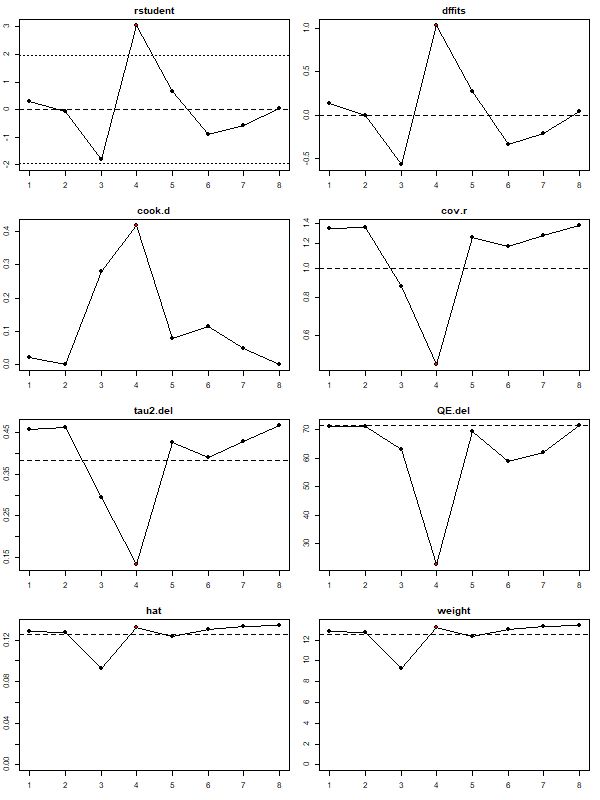
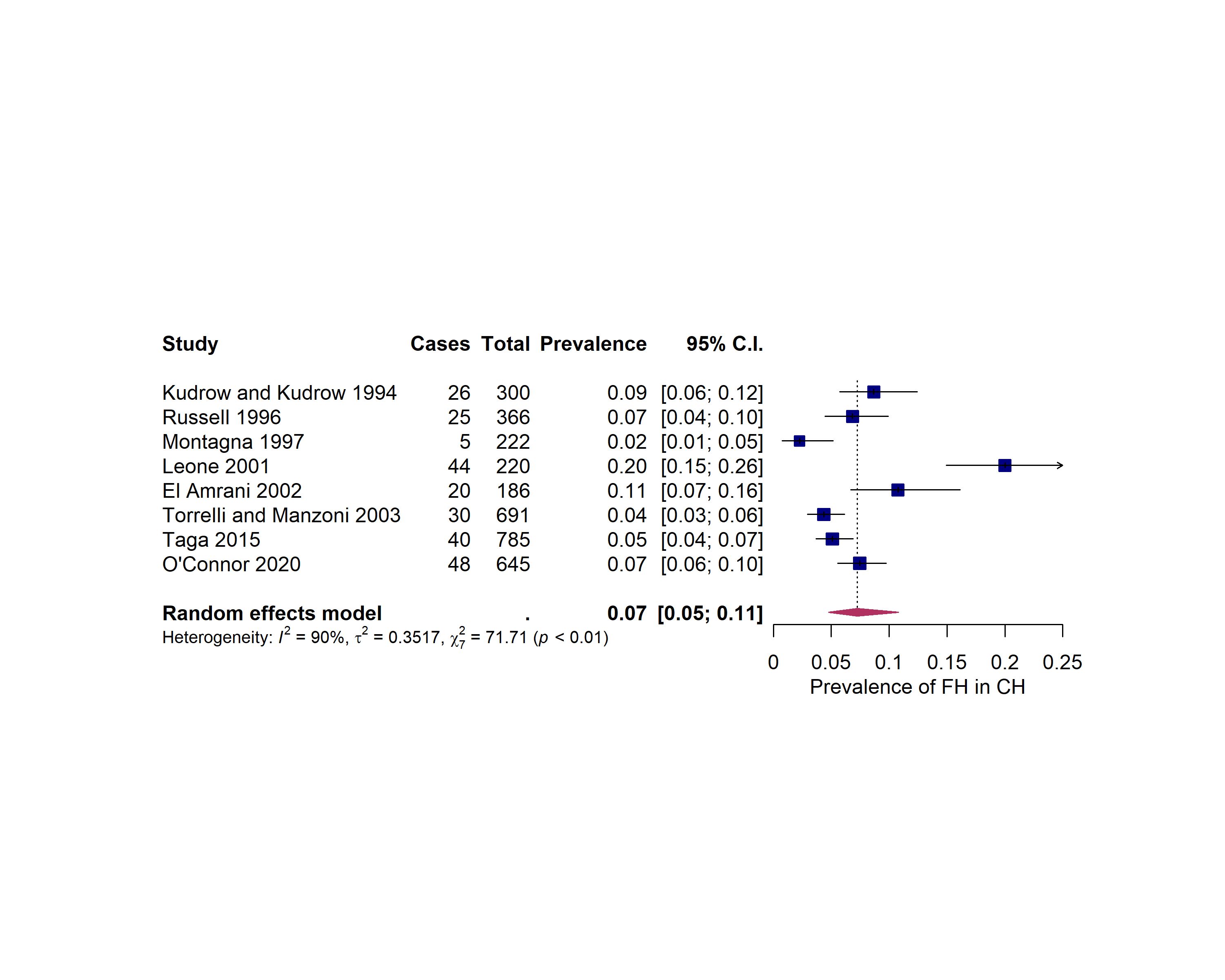
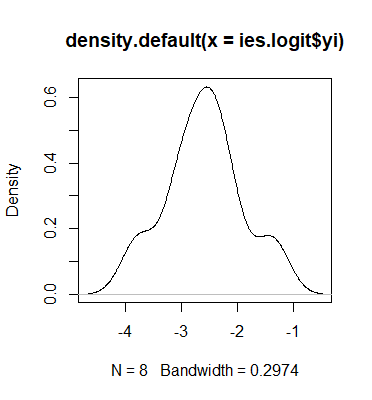
Of the seven identified studies, we extracted the total number of affected probands with a first or second degree relative with a clinical diagnosis of cluster headache and the total number of cases in the study [13, 28-32]. The raw/direct proportions were calculated and the distribution of untransformed, logit and double-arcsine transformed proportions were compared. The distributions of the proportions were assessed for normality using density plots and tested using the Shapiro-Wilk test. Logit-transformed proportions most resembled a normal distribution therefore, this transformation was used for the analysis. Due to high inter-study variation and high I2, a random-effects model was fitted for estimation of family history in CH. After fitting a model to all relevant studies, leave-one-out analyses (LOO) and accompanying diagnostic plots were used to identify influential studies including: externally studentized residuals, difference in fits values (DFFITS), Cook’s distances, covariance ratios, LOO estimates of the amount of heterogeneity, LOO values of the test statistics for heterogeneity, hat values and weights. Briefly, each study was removed one at a time, and the summary proportion is re-estimated based on the remaining n-1 studies. Studies with a statistically significant influence on the fitted model were removed as outliers and the model was re-fitted. All data analysis and visualisation was performed using the R statistical environment (version 3.6.1, 2019-07-05) using the “metafor" and "meta” packages. The analysis was performed as outlined by Wang [33].
We performed a gender-segregated analysis that included all studies from our initial analysis which also reported the prevalence for males and females separately. In total, studies had gender segregated numbers: Kudrow and Kudrow (1994), Russell (1996), Leone (2001), El Amrani (2002) Taga (2015) and our unpublished cohort: O’Connor (2020). We represented each study with a male and female estimate of family history prevalence. Leone (2001) was identified as an outlier in our initial analysis. We continued to exclude this study for two reasons: our method of analysis results in two separate entries per study (one male, one female), causing influential studies to be over-represented which may skew outlier analysis, and secondly, these estimates are not truly independent. Based on the identified literature, we chose not to assume a common between-study variance component across males and females, therefore, we did not pool within-group estimates of τ2. Additionally, there were five studies per subgroup, allowing a moderately stable estimate of τ2 within each subgroup. We, therefore, used a mixed-effects model whereby, all summary effect sizes where calculated using separate τ2 within each subgroup (males and females), then two separate random effects models were fitted. We then combined the estimated statistics from each model and fitted a fixed-effect model as outlined by Wang [33].
{kind=link}
{kind=link}
{kind=link}