This was the first study conducted in Iran to evaluate ciliary ultrastructural defects among patients presenting with symptoms attributable to PCD. Early diagnosis of PCD is of great importance as appropriate clinical intervention and early treatment prevent permanent bronchiectasis and other insidious lung tissue damage (9).
According to the European Respiratory Society Guidelines for the diagnosis of primary ciliary dyskinesia, it is highly recommended that patients with recurrent wet cough, chronic rhinitis, persistent middle ear disease, congenital heart disease, neonatal respiratory infections in infants and a history of intensive neonatal treatment be screened for PCD. In addition, PCD patients' siblings should also undergo PCD investigations (10, 11). The most prominent symptoms among patients were bronchiectasis (39%) and persistent sinusitis (34%). However, in the PCD group, persistent respiratory infection was even greater than those symptoms reported (50%).
PCD and SCD may have similar symptoms, but TEM findings are permanent and seen in most of the cilia in PCD patients. Secondary changes, however, could be the result of former infections and would recover by the time or culture of the sample (6, 12, 13). Compound cilia (41.4%) and extra-tubules (44.3%) are examples of SCD identified in almost half of the sample population (Figure.2).
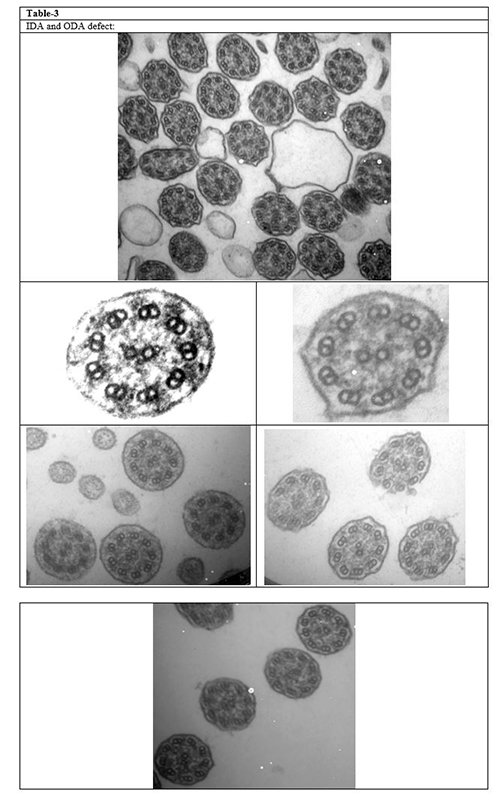
Furthermore, some changes, such as microtubular disorganization and central pair abnormalities, may be common between PCD and SCD. Therefore, to confirm this diagnosis, they should present with other specific PCD criteria. Repeating the biopsy and considering a sufficient healthy interval before sampling also help to differentiate between PCD and SCD more precisely (14). IDA defect is also among the overlapping appearance seen in almost 30% of our samples, probably due to the difficulty of seeing IDA by TEM (15-17). (Table-3) (Figure.3).
It is therefore highly suggested that the biopsy be iterated specifically for this group (18). In addition, in the event of an isolated IDA defect, the cultivation of the sample may result in a reversal and therefore exclude the diagnosis of PCD (6). Likewise, considerable attention must be paid to the ultrastructure at the tip and base of the cilia to prevent misinterpretation as ultrastructural defect (14).(Figure 4).
To date, PCD diagnosis remains a significant medical challenge in resource-limited regions. Although TEM was previously thought to be a gold standard test, there is currently no stand-alone PCD test and there are also a variety of diagnostic approaches in different countries based on their local guidelines (19).
Several techniques are required to confirm PCD diagnosis, as well. Saccharine testing was previously done for PCD screening (20), although this is not reliable anymore (20). To date, nasal nitric oxide (nNO) and high-speed video microscopy analysis (HSVA) have been used in combination with TEM to confirm a PCD diagnosis based on local diagnostic algorithms. However, the European Respiratory Society Guideline (10) labels nNO (for patients under the age of 6 years) and HSVA as a "weak recommendation" and still strongly advocates TEM. Due to the lack of a local guideline in our region, we recommend that TEM be a reliable tool because of its high specificity. However, up to 30 percent of PCD patients have normal TEM results (14). Furthermore, by using TEM alone, there is no confirmed diagnosis for patients with" Class 2 "defects (indicate PCD). We therefore suggest that other tests should be performed for these patients, along with TEM repeat or sample cultivation, to make further decisions (14). Further studies are needed to establish a local guideline in western Asian countries.
These patients would have a normal joyful life only if they are diagnosed on-time and given proper antibiotic treatment in each respiratory infections. Regular physiotherapy is useful, as well (21) On the other hand, recurrent infections will result in respiratory complications, including recurrent pneumonitis, bronchiectasis, parenchymal fibrosis, hypoxemia induced by ventilation / perfusion mismatch and right ventricular failure, if they remain undiagnosed. Hence, early diagnosis would prevent irreversible consequent complications caused during clinical course and also reduce the burden of disease and its great cost for the health system (22).
Our work has led us to conclude that among suspected PCD patients the most common ultrastructural ciliary defects were extra-tubule and compound cilia. However, the most prevalent hallmark diagnostic defects were ODA and IDA defect among PCD patients. Further studies are needed to establish a local guideline in western Asian countries.
{kind=link}