The lung and gut microbiome axis has increasingly been studied over the last decade to elucidate the relationship between microbiome dysbiosis and immunity in the lung (16-22). The gut-lung microbiome axis has been proposed and studied for its ability to help regulate the immune system (13, 22, 23). Because there are a vast number of microbes residing in the gut, there is no shortage of microorganism-associated molecular patterns (MAMPs) as well as pathogen-associated molecular patterns (PAMPs) that can initiate in the gut and alter immune functions in the lung (24). MAMPs and PAMPS are able to activate Toll Like Receptors (TLR) on dendritic cells, T cells, epithelial cells, macrophages, and B cells. This activation of TLRs can change cytokine, chemokine, and antibody production in the lung, all of which have been shown to be important in viral clearance for RSV (25, 26).
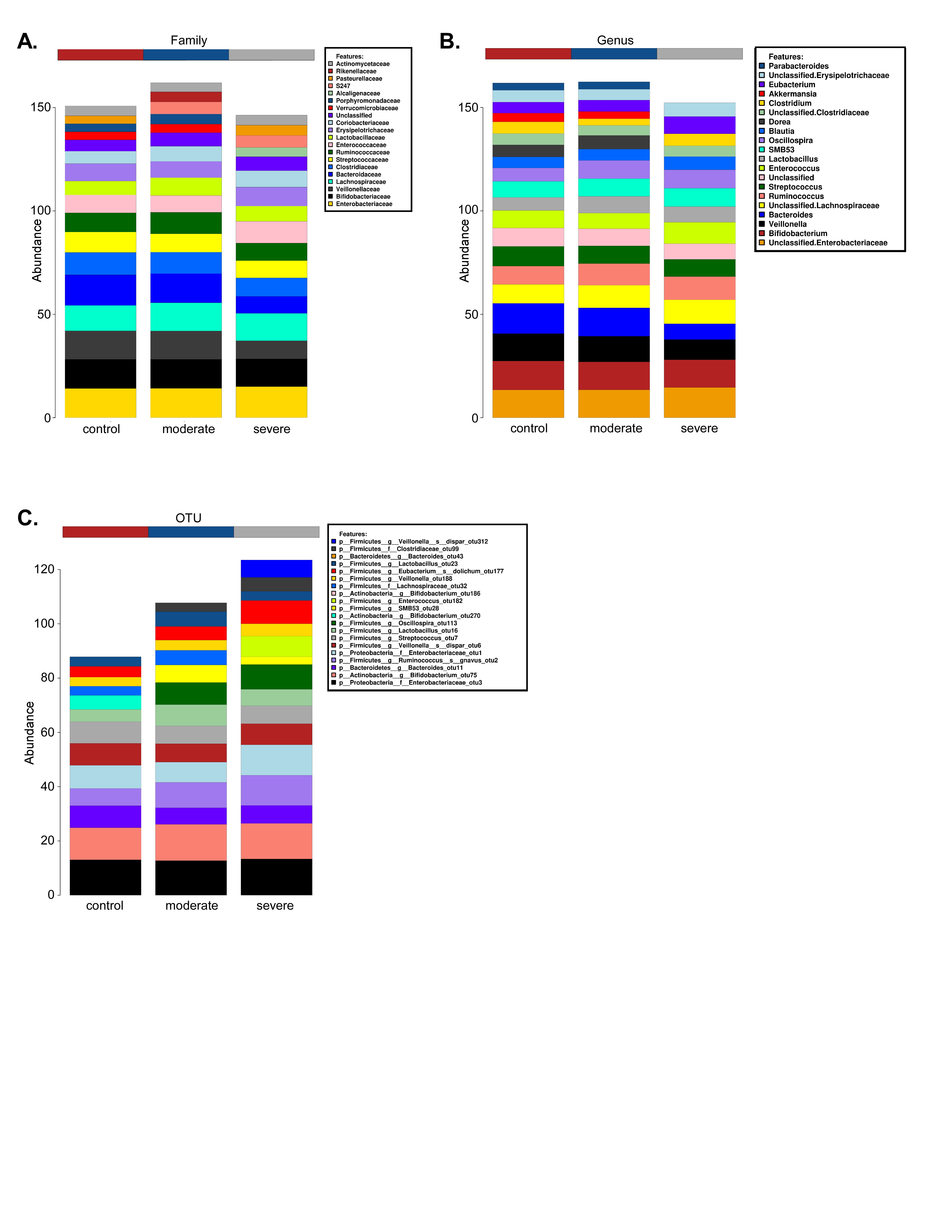
Studies have shown associations between bronchiolitis and the gut microbiome in infants, along with associations between RSV and the gut microbiome of mice. In infants, these studies demonstrated that there was a Bacteroides-dominant profile that was associated with a higher likelihood of bronchiolitis (27). In mice, there was a significant increase in Bacteroidetes and a decrease in Firmicutes phyla abundance (13). However, to our knowledge, our study is the first to directly investigate the role of gut microbiota in RSV disease severity in infants. Our findings indicate that between RSV infected patients and control patients there are no significant changes in the abundance of microbes in the gut (Figure 2A, B), but there is a significant change in gut microbial composition between RSV infected patients and control patients (Figure 3A).
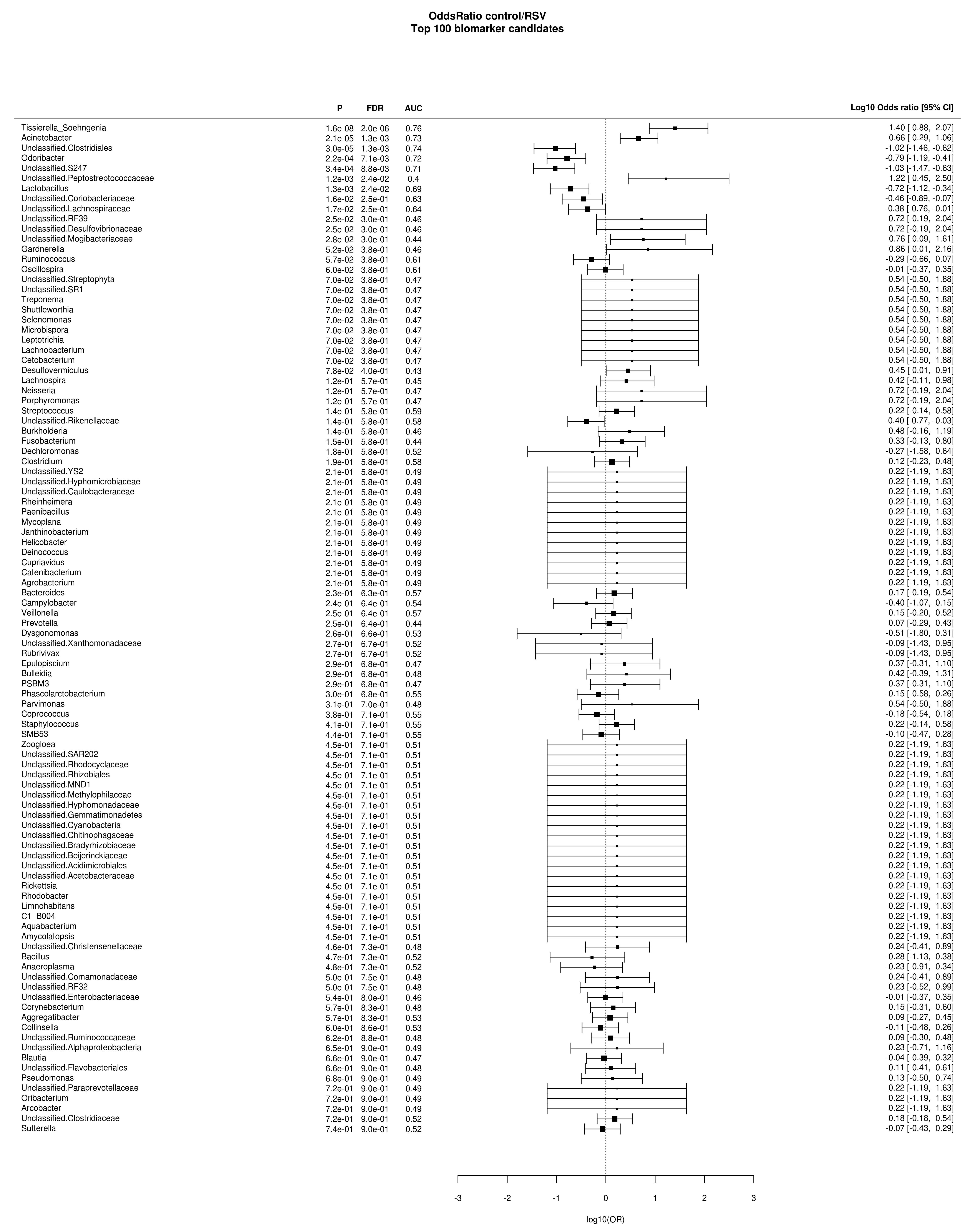
Furthermore, there were significant enrichments in the families S24_7, Clostridiales, Odoribacteraceae, Lactobacillaceae, Actinomyces using LEfSe and ANOVA with BH correction between these RSV and control patients. Likewise, our data indicates that when looking at severity (PICU vs. Non-PICU vs. Control), there is only a slight decrease in commensal microbial abundance across the patient groups (Figure 2C, D). We do, however, see separate phylogenetic clustering between the severe and moderate patients and separation from the control patients (Figure 3B). This clustering was shown to be dependent upon Enterococcus, Lactobacillus, Oscillospira, Odoribacter, Tissierella Soehngenia, and S24_7 (Figure 4). The LEfSe analysis showed us 6 bacterial OTUs that were enriched in the severe group when compared to the moderate and control groups. Specifically, a significant increase in S24_7 OTU 191 coincided with severe versus moderate RSV (Figure 5D). This data suggests that the bacteria that are driving these differences are encompassed within the Firmicutes and Bacteroidetes phylum but are varied at the family and OTU levels illustrating unknown factors contributing to this dysbiosis of the gut microbiome. Our study demonstrates that the gut microbiome diversification is associated with RSV disease severity and suggests that altering the gut microbiome may have clinical relevance.
Despite the fact that S24_7 has been shown to make up a significant portion of the mouse and human intestinal microbiome (13, 28, 29). A study characterizing 30 population genomes of S24_7 found that 20 of the 30 populations genomes contain a metalloprotease belonging to M6 peptidase family. Peptidases within this family exhibit antimicrobial capabilities as well as degradation abilities for extracellular matrices (ECM). In addition to M6 peptidase in their genomes, 11 of the 30 populations of S24_7 contained IgA degrading peptidase sequences in their genomes (peptidase family M64). This could be crucial to the microbiome’s interaction with RSV severity as it has been shown that IgA is vital for mucosal defense in RSV infection and aids in protection to upper respiratory tract infections (30-34). These mucosal antibodies have, similarly, been shown to protect human adults from experimental RSV infection (35, 36). Therefore, IgA is important for protection and disruption of memory IgA can contribute to severity and reoccurrence of RSV. While it is enticing to speculate that elevations in M6 peptidases due to enrichment of S24_7 family members leads to degradation of RSV specific IgA and disease severity, it is yet to be determined whether a gut microbial profile low in diversity and enriched in S24_7 is the cause, or result, of severe RSV disease. Mechanistic studies need to be done in order to address this important question. It is possible that by elucidating the mechanism of S24_7 in RSV disease severity therapeutic targets could be identified.
Our findings highlight that there is a correlation between RSV infection and dysbiosis of the gut microbiome. We identified disruptions in the abundance of microbes in patients with severe RSV disease as well as characteristic microbiome shifts in all RSV patients. We identified that there were 6 specific, enriched microbes associated with RSV severity. Together, our findings identified changes in phylogenetic diversity in RSV patients and identified specific microbes associated with severity of disease. However, there were limitations to this study. One of the limitations of this study is the small sample size, particularly for severe RSV patients. It is also noteworthy that this study was conducted in Memphis, Tennessee where there is a socioeconomic and racial skew in patient demographics that can be a limitation to the extrapolation of these studies across sites. It is unclear if the changes in gut microbiota are causal or correlated with RSV (or hospitalization). Further studies need to be done to characterize the change in gut microbiota of RSV patients fully. Future work will include additional patient recruitment to more precisely define a gut microbial profile associated with severe RSV disease. These studies could lead to the development of logistic regression models to predict infants at high risk for severe RSV disease based on gut microbiome.
{kind=link}
{kind=link}
{kind=link}