Objective
Primary objective
The primary objective is to identify if CFT is more efficacious than combined Core Training exercise and manual therapy (CORE-MT) for patients with non-specific chronic low back pain in terms of pain and disability two months after the first session.
Secondary objective
The secondary objective is to identify if the effects observed two months after the first session can be sustained over six and twelve months and also to investigate the global perceived effect, patient satisfaction, mediators as well as moderators and predictors of treatment effect, which is assessed two, six and twelve months after the first session.
Design and setting
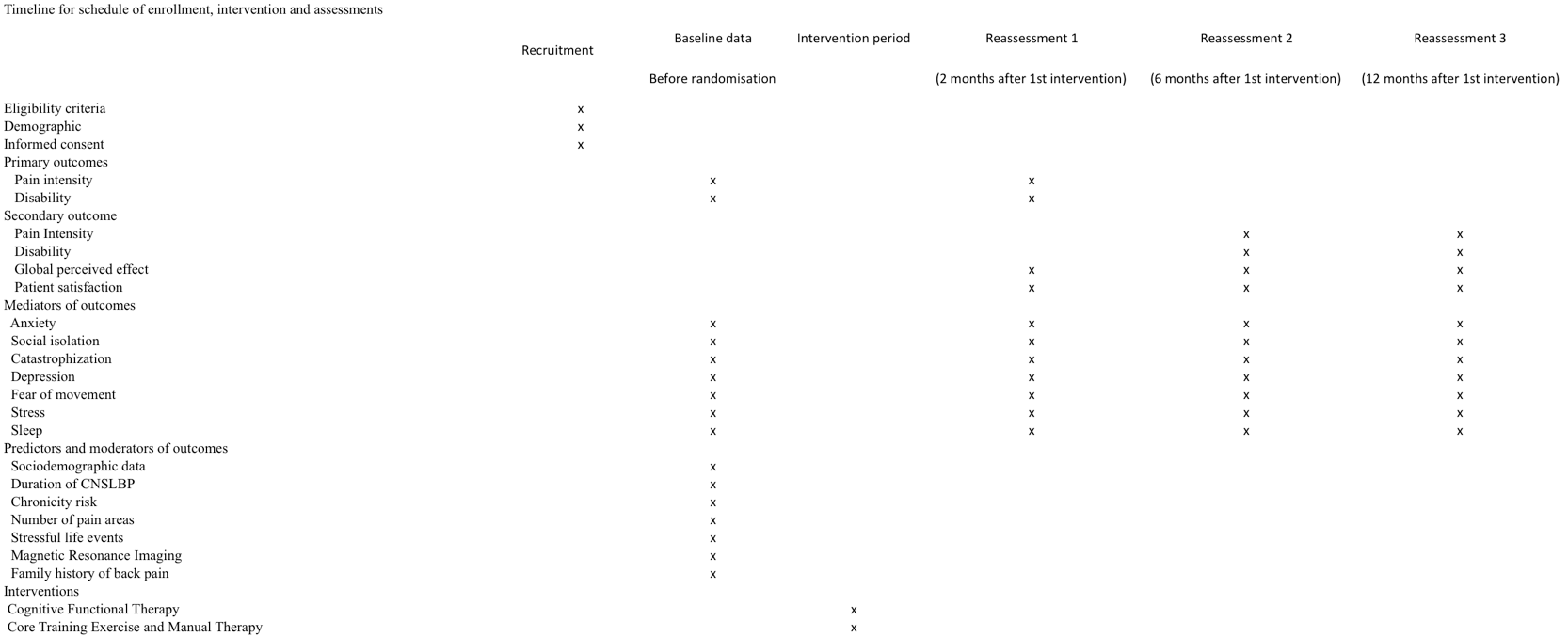
A randomized controlled trial with blinding of assessors and allocation in parallel groups will be applied (Fig. 1). The study will be conducted in a private clinic in Campinas, São Paulo, Brazil.
Recruitment and participants
We will recruit patients of both sexes who are seeking treatment for low back pain (with symptoms for at least three months) (1). A physiotherapist who is not aware of the treatment allocation, since randomization will be performed after the baseline assessment, will screen the patients to confirm eligibility described in table 1. This screening procedure consists of collecting a brief patient’s history and applying a disability-related questionnaire that is an inclusion criterion for the study. Participants who meet the eligibility criteria will be recruited but will be given the option to be or not to be part of the study. Eligible patients will be informed about the study’s objectives and procedures, and it will be clear that there are two groups of active interventions and that is not known which intervention is superior. To guarantee that the treatment expectation is evenly balanced between the groups, the participants will not know the study hypothesis. If the patient agrees to participate in the study, he/she will sign a consent form, and the physiotherapist will collect data for the baseline immediately.
| Table 1. Inclusion and exclusion criteria for study participation | |
| Inclusion criteria | Exclusion criteria |
| Aged between 18 and 65 | Primary pain area is not the lumbar spine (from T12 to buttocks) |
| Chronic low back pain for at least 12 weeks duration | Leg pain as the primary problem (e.g., nerve root compression or disc prolapse with true radicular pain/radiculopathy, lateral recess or central spinal stenosis) |
| Independently mobile (with or without aids) |
| Be able to speak and understand Portuguese well enough to be able to complete the questionnaires independently | Pain relieving procedures such as injection-based therapy (e.g., epidurals) and day case procedures (e.g., rhizotomy) in the past 3 months |
| | Pregnancy |
| | Rheumatological/inflammatory disease (e.g., rheumatoid arthritis, ankylosing spondylitis, psoriatic arthritis, lupus erythematosus, Scheuermann’s disease) |
| | Progressive neurological disease (e.g., multiple sclerosis, Parkinson’s disease, motor neuron disease) |
| | Scoliosis (if considered the primary driver of pain) |
| | Unstable cardiac conditions |
| | Red flag disorders like malignancy/cancer, acute traumas like fracture (less than 6 months ago) or infection, spinal cord compression/equine tail. |
Treatment allocation and randomization
Randomization will be computer-generated by the main researcher who will not be involved in the recruitment and treatment of patients. This process will occur after determining if the participant meets the inclusion criteria. The allocation of the participants will be performed using secret numbers sequentially ordered in opaque envelopes. The envelopes will be opened sequentially by the physiotherapists responsible for the interventions. Both arms include active treatments and participants will not know whether they are in the experimental group or control group.
Intervention
The patients randomized in the CFT group will be treated by a newly graduated physiotherapist with one year’s clinical experience in CFT. She attended two CFT workshops with two of the tutors of the method and completed 106 hours of training including workshops, patient examinations and a pilot study with the supervision of a physical therapist with more than three years of clinical experience in CFT. Patients in the CORE-MT group will be treated by a physical therapist with five years of clinical experience in manual therapy and Core Training exercises. For both groups, the treatments will be five one-hour sessions for an eight-week intervention period, on a weekly basis for the first two weeks and then a session every two or three weeks. The patients will always be treated by the same physical therapist who will not be involved in the reassessments of patients. The assessment of treatment fidelity will be performed by in vivo observations as well as video recording during the pilot study and along the trial. Also, regular meetings to discuss these clinical cases will be performed.
The participants from both groups are encouraged to remain active. The two interventions involve movements and home-based exercises. Physiotherapists from both arms will receive weekly feedback from the patients (e.g.: exercise frequency, number of repetitions and sets). However, we haven’t quantified the feedback because our aim was to test the intervention in a pragmatic way. This is in order to represent the reality of intervention in clinical practice, where there are patients who adhere to the orientation and those who do not. The aim of our experimental intervention, CFT, is to change maladaptive behavior and stimulate a lifestyle change. Although the home-based exercises are prescribed, we expect that patients’ improvements will be more mediated by functional behavior change in their daily lives than adherence to prescribed exercises.
Experimental intervention: Cognitive-Functional Therapy (CFT)
There will be four main components in the intervention, following the protocol used by O’Keefe et al.(12). These will be the following:
-
The cognitive component will focus on identifying the factors that contribute to pain during examination. This will include discussion on the multidimensional nature of persistent pain about individual beliefs, and how emotions and behaviors (movement and lifestyle) can reinforce a vicious cycle of pain and disability.
-
Specific Functional training is designed to normalize maladaptive or provocative movement and posture. For this, we will ensure the patient feels safe, with body relaxation and exposure to valued activities that are painful, feared or avoided.
-
Functional integration directed to activities of daily life such as rolling, bending and sitting. This will vary between individuals but should integrate new behaviors with valued goals, gradual exposure into daily life, reduce threats and conditioning when indicated.
-
Physical activity and lifestyle. Patients will be advised to gradually increase physical activity based on their preference, and also focus on sleep hygiene, stress and pain self-management strategies.
Treatment with CFT will be individualized, and the physiotherapist will listen to the entire patient pain history, and the intervention will be focused on individual needs. The first session consists of the evaluation process integrated with the beginning of the treatment. It includes a thorough history and physical examination, in order to identify factors that potentially mediate pain and disability (12, 15, 16). A timeline of the pain history recalling bio-psycho-social factors that may have played a role in the arising and persistence of the symptoms can help patients making sense of their non-specifc persistent pain and disability.
The reflexive listening aims to identify the context, area and characteristics of pain, level of disability, beliefs, physical factors, coping strategies, lifestyle factors, goals, values and imaging exams analysis. Listening to the patient’s history is key and will contain elements such as empathy, mirroring, reflective issues, and reinforcement of positive behaviors. It is because of this active listening that is possible to identify a path of recovery through what is identified as changeable. Afterwards, a summary of what was discussed will be recorded.
The physical examination consists of examining pain responses, analyzing functional behavior through observation, guided behavioral experiments, modifiability of behaviors and pain controllability linked to functional goals. The level of activity will also be assessed, such as their ability to relax the trunk muscles and normalize posture and provocative movement behavior (12, 13, 15). Where a maladaptive behavior is identified, then an alternative strategy of movement is implemented. This component of the treatment is called exposure with control (11).
Some exercises with these more relaxed and natural movements and instructions aimed at patient functional recovery will be filmed or written when deemed appropriate by the physiotherapist and/or requested by the participants so that they can perform them at home.
With a new movement strategy implemented, subsequent sessions will be to explore ways of generalizing learning and integrating into daily activities, as well as gradually progressing to the most feared or avoided tasks. Initially these patients will be encouraged to practice daily in order to achieve progress and become capable of re-engaging in a physical activity of their choice. It is also during the sessions that patients develop an understanding of the contexts in which pain flare-up happens; therefore, positive coping strategies can be determined and discussed at this point.
Control intervention: Core Training exercise and manual therapy (CORE-MT)
The participants assigned to the comparison group will be treated with a strengthening program to maximize static core muscle endurance and dynamic core stability, based on McGill core exercises (17). The approach consists of trunk, abdominal and pelvic strengthening in different functional positions and progressively in relation to difficulty and intensity. The exercise will include activation of core musculature in static positions and during cycles of flexion and extension in quadruped position, maintenance of core control while performing arm and leg movements, during hip and multiplanar movements and activation of the hip musculature while maintaining lumbar and pelvic control. These exercises are performed with resistance and on unstable surfaces according to the progress of each patient (18).
The physiotherapist of this group will provide instruction, demonstration and individual feedback for the exercises. In addition, mobilization and joint manipulation will be used pragmatically when necessary. The patients in this group will receive exercises to perform at home, but not related to CFT exercises (19).
Outcome measures
All outcome measures will be self-reported and will be conducted pre-intervention, post-intervention, as well as six and twelve months after intervention. The primary outcomes will be pain intensity and disability associated with low back pain measured post-intervention (two months after first intervention session). The secondary outcomes will be pain intensity and disability assessed six and twelve months after the first intervention session and both global perceived effect and patient satisfaction assessed two, six and twelve months after intervention.
-
Pain intensity will be measured with the Brazilian version of the Numerical Scale of Pain 11 points (END) (20). The END scale ranges from 0 to 10, where 0 is "no pain" and 10 is "the worst pain imaginable." Participants will be asked to answer about their pain levels based on the last seven days.
-
Disability associated with low back pain will be assessed by the Oswestry Disability Index (ODI). It is a tool widely used in research and clinical practice to assess disability related to low back pain. This questionnaire has 10 items (0–5 points each) related to activities of daily living that patients with low back pain have more difficulties performing. The sum of the scores of items is multiplied by two and the percentage of disability varies from 0 to 100%. The ODI has been properly translated and culturally adapted into Portuguese, and their measurement properties tested in patients with low back pain in Brazil (21).
-
Global impression of recovery will be assessed by the Global Perceived Effect Scale (GPES) which is an 11-point scale ranging from − 5 (vastly worse), through 0 (no change) to + 5 (completely recovered) (22). For all measures of the GPES at all follow-ups, participants will be asked: "Compared to when this episode first started, how would you describe your low back these days?” A higher positive score indicates greater recovery and a negative score indicates worsening of symptoms.
-
Patient satisfaction will be assessed by the patient satisfaction questionnaire (23).This is a simple questionnaire from 1 to 5 asking the patients how satisfied they are with their treatment: 1 = satisfied, 2 = just a little satisfied, 3 = neither satisfied nor dissatisfied, 4 = just a little dissatisfied, 5 = dissatisfied.
Mediators of outcome
The potential mediators of the outcome will be assessed two, six and twelve months after randomization with brief screening questions for anxiety, social isolation, catastrophization, depression, fear of movement, stress, and sleep (24). These brief questions are comparable to full-length validated questionnaires.
-
Anxiety will be evaluated by the question “Do you feel anxious?” with the response options ranging from “Not at all” = 0 to “Quite anxious” = 10.
-
Social isolation will be evaluated by the question “Do you feel socially isolated?” with the response options ranging from “Not at all isolated” = 0 to “Quite isolated” = 10.
-
Catastrophization will be evaluated by the question “When I feel pain, it’s terrible and I feel it’s never going to get any better” with the response options ranging from “Never do that” = 0 to “Always do that” = 10.
-
Depression will be evaluated by the question “During the past month have you often been bothered by feeling down, depressed or hopeless?” with the response options ranging from “Never” = 0 to “All the time” = 10.
-
Fear of movement will be assessed by the question “Physical activity might harm my back” and the response options will range from “completely disagree” = 0 to “completely agree = 10.
-
Stress will be evaluated by the question “Do you feel stressed? and the response options will range from “completely disagree” = 0 to “completely agree = 10.
-
Sleep will be evaluated by the question "Did you have sleep problems last month?" based on Subjective Health Complaints Inventory (25). The response options will be “Not at all” = 0, “A little” = 1, “Some” = 2, and “Serious”
Timing of outcome measurement
Pain intensity, disability and global impression of recovery, satisfaction and potential mediators of the outcomes, anxiety, social isolation, catastrophization, depression, fear of movement, stress, sleep problems, will be collected at baseline (except satisfaction). Patients will receive a call by a blinded assessor to complete the questionnaires post- intervention at two months and at six and twelve months.
Predictors and potential moderators of outcome
1) Sociodemographic data: participants’ age and sex will be obtained.
2) Duration in months of CNSLBP will be obtained through the question: "How long have you had low back pain?"
3) Chronicity risk will be assessed through 10 items of the short version of Örebro Screening Questionnaire and also through the Brazilian version of Start Back Screening Tool (26, 27).
4) Number of areas of pain will be obtained through the number of marks filled on the diagram which contains forty nine different areas (28).
5) Stressful life events will be obtained through closed questions with dichotomous answers (yes and no), covering the following: serious illness which resulted in distance from usual activities; hospitalization due to illness or accident; close relative`s death; severe financial problems; forced change of residence; separation/divorce; physical aggression; and robbery/theft (29).
6) Magnetic Resonance Imaging: participants will be asked: "Have you ever undergone an MRI for the lumbar spine?" Answer options: yes or no.
7) Family history of back pain: the following question will be asked: "Do you have any relatives suffering from back pain?" Answer options: yes or no.
The sociodemographic (1) information, pain duration (2), predictors and moderators will be obtained only at baseline. Mediators will also be obtained for all reassessments (two, six and twelve months after the first session). The average time spent to fill the baseline questionnaire is 25 minutes. The average time to answer the follow up questionnaire by telephone is 10 minutes.
Blinding
The clinical outcomes will be obtained in the evaluations carried out by two blinded assessor (physiotherapists) two, six and twelve months after the first intervention session. Blinded assessors were trained by the principal researcher during a pilot study. They will not be treating any of the participants nor be aware of their group allocation or receive any information regarding the treatment arm of the patients. Also, both blinded assessors will not have access to the place where the treatment is being delivered or the waiting room. The statistician conducting the primary data analysis will also be blinded to group allocation. Due to the nature of the interventions, it will not be possible to blind the participants and the therapists.
Statistical analysis
Descriptive statistics will be used to describe the characteristics of the participants in both treatment groups. The intention to treat analysis will be performed using linear mixed models to compare the mean differences in pain intensity, disability and global perceived effect between the intervention arms.
The analysis will be conducted by a statistician who will receive the encoded data. Analysis of secondary outcomes will involve linear and nonlinear models mixed for continuous and categorical variables respectively.
Variable selection techniques will be used to identify the most parsimonious combination of the characteristics of the participants for inclusion as explanatory variables in each model. The analysis of the potential mediators’ effect on the treatment will be performed using causal mediation methods described by Imai and colleagues (30).
The baseline variables will be evaluated as predictors and moderators of treatment including terms and interaction models. A level of statistical significance of 5% will be used in the analysis. All analyses will be performed using the RStudio version 0.99.486.
Sample size estimation
The required sample size for this study is 74 per group to detect a mean difference of 5.0 for disability and 1.0 for pain intensity between the two intervention arms, assuming a standard deviation of 10.0 for disability and 2.0 for pain with an alpha error of 5%, a power of 80% and a possible 15% loss to follow-up. The statistical power of our study will be able to detect a mean difference lower than the minimum important change (MIC) for pain (Numerical Pain Rating Scale score of 2 point) and lower than the MIC for disability (Oswestry Disability Index score of 10%).
Limitations
Having a single therapist delivering the treatment in each arm can help make treatment consistent, however it can decrease the generalizability.
{kind=link}