Study Population
A retrospective cohort study of all pregnant women who visited the CMV clinic in a single university affiliated tertiary medical center, between 2012 and 2016, and were diagnosed with primary CMV infection during pregnancy. Women were categorized according to CMV urinary excretion: positive urinary excretion group and negative urinary excretion group at time of diagnosis. We excluded women who were diagnosed with non-primary CMV infection, periconceptional CMV infection, multiple gestations and women who participated in a parallel interventional trial for CMV prevention. In addition, women who did not undergo amniocentesis or whose neonatal electronic health record did not contain information on CMV urinary analysis, were also excluded.
Definitions
Primary CMV infection was defined in women who underwent CMV IgG seroconversion, according to their serology analysis prior to and during pregnancy. If prior IgG status was unknown, IgG avidity was measured to ascertain the acuity and timing of the infection [13-14,19-20], and to exclude any suspected peri- or pre-conceptional infections. In some women with IgG seroconversion but otherwise borderline serology patterns, maternal symptoms were also taken into account in determination of primary infection. CMV DNA urine excretion analysis was used to stratify women to the abovementioned study groups.
Congenital CMV infection was defined by positive PCR for CMV DNA in amniocentesis that was performed after 21 gestational weeks and at least 7 weeks after the onset of maternal infection [21], or by detection of CMV in neonatal urine analysis, which was performed immediately after birth. Congenital CMV disease was defined for any fetus with sonographic or MRI findings that are considered suggestive of a congenital disease, as well as for any neonate with signs of sensorineural hearing loss, as evaluated by a post-partum brainstem Evoked Response Audiometry (BERA), preformed shortly after birth.
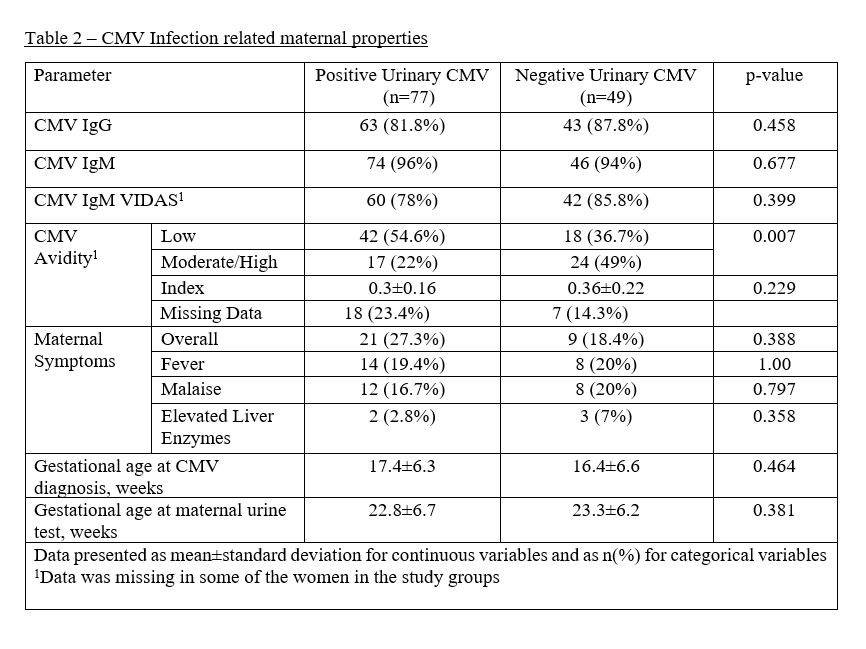
Maternal acute CMV infection symptoms were collected as well, including mononucleosis-like symptoms such as fever and malaise, and elevated liver enzymes [22].
Data Collection
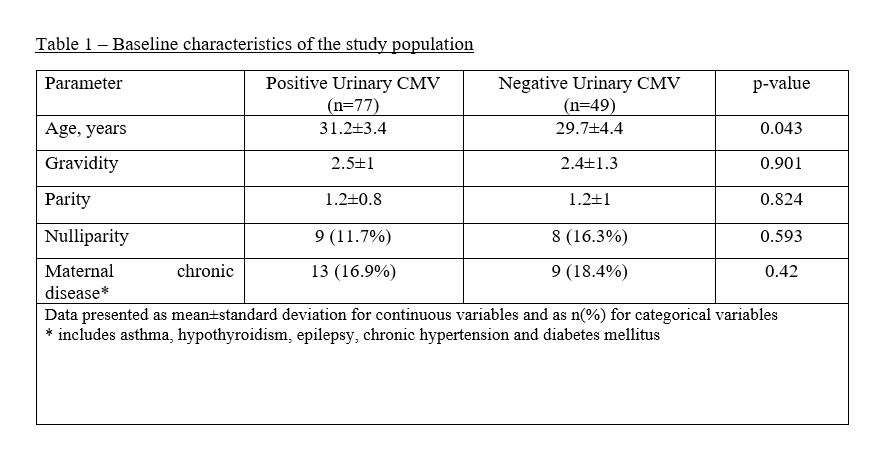
Data was retrieved from the computerized comprehensive database of our CMV Clinic. The following demographic and CMV related maternal properties were recorded: age, gravidity, parity, any maternal chronic diseases, CMV serology status during and prior to conception (including IgG, IgM, IgM VIDAS and IgG Avidity), urinary qualitative PCR for CMV detection, maternal symptoms (fever, malaise) and laboratory results (Aspartate Transaminase [AST], Alanine Transaminase [AST]) during acute CMV infection, gestational age at CMV infection diagnosis, as well as gestational age at urine analysis and amniocentesis.
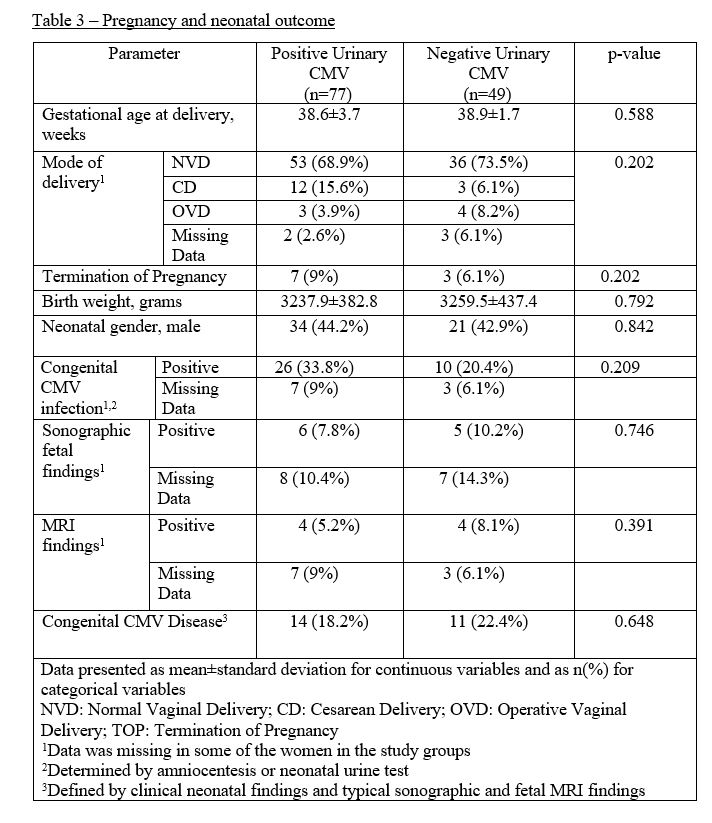
The following obstetrical, fetal and neonatal parameters were recorded: gestational age at delivery, mode of delivery, birth weight, gender, PCR results for CMV DNA in amniocentesis, neonatal urine analysis via PCR for CMV detection and neonatal BERA test.
Imaging studies are routinely performed among primary CMV infected women in order to assess the probability of symptomatic congenital disease of the fetus and newborn. We collected sonographic and brain MRI fetal findings which are typical (but not pathognomonic or specific) for congenital CMV disease, including bilateral periventricular calcifications (hyperechoic foci), intraventricular adhesions, cerebral ventriculomegaly, microcephaly, fetal growth restriction, hyperechogenic fetal bowel, hepatic calcifications and hepatosplenomegaly [21, 23-27].
Outcome Measures
The primary outcome measures of the study were defined as congenital CMV infection, determined by either CMV-positive amniocentesis or neonatal urine and as congenital CMV disease, determined by typical sonographic or MRI findings and/or by neonatal abnormal BERA test results. The secondary outcomes were congenital CMV disease rates, and congenital CMV infection rate when compared between symptomatic and asymptomatic women.
Statistical Analysis
Statistical analysis was generated using SAS Software, Version 9.4. Continuous variables were presented by mean and standard deviation. Categorical variables were presented by number and percentage. Two-sided p values less than .05 were considered statistically significant.
Ethics
The study was approved by the local Institutional Review Board at Rabin Medical Center, approval no. RMC-13-0237.
{kind=link}
{kind=link}
{kind=link}