3.1 Baseline Characteristics
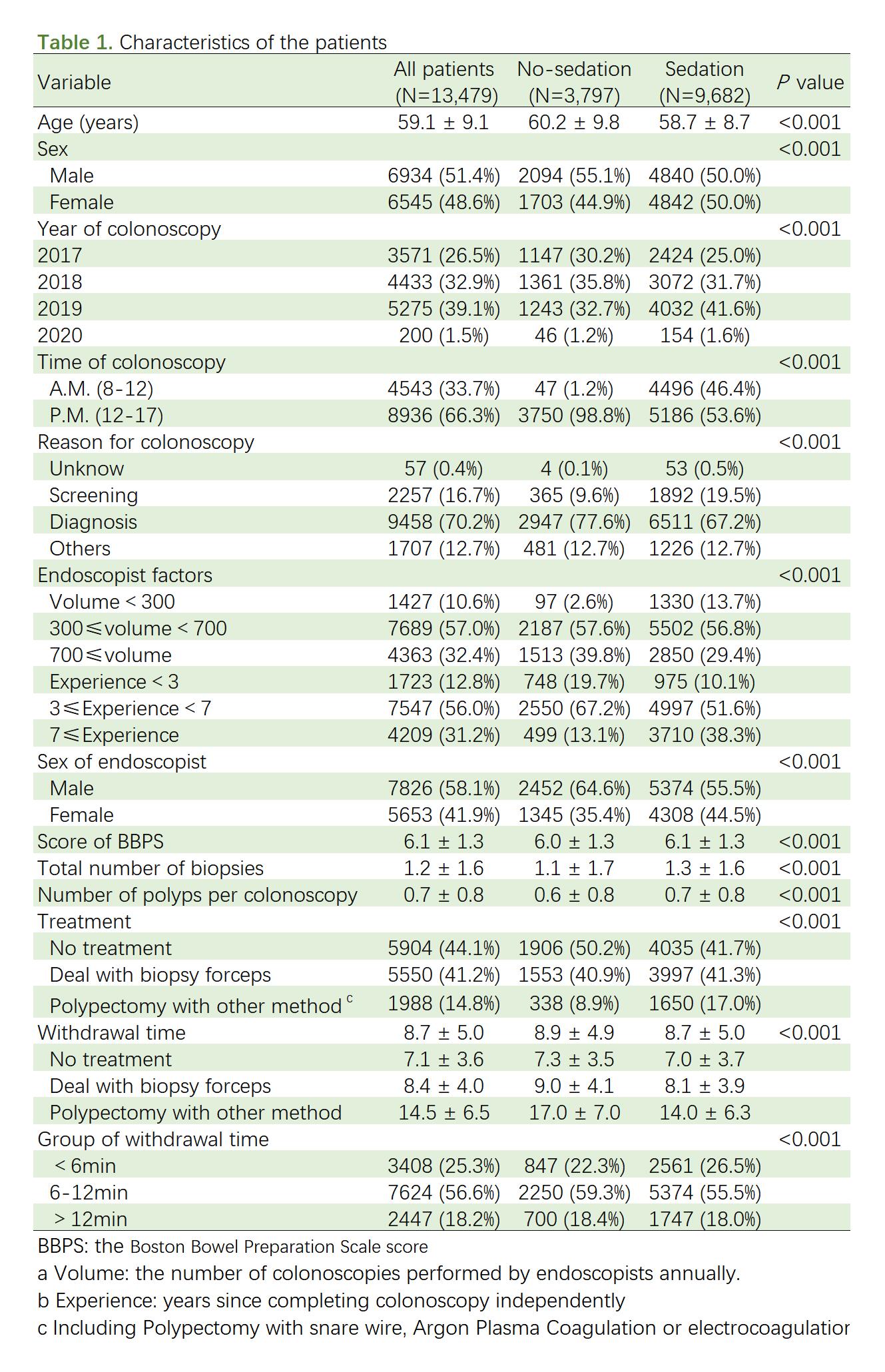
Overall, we identified 20319 ambulatory patients who underwent colonoscopy between January 1, 2017, and January 31, 2020. 6840 cases were excluded according to exclusion criterion. A total of 13479 patients were finally included for final analysis in our study, of which 9682 (71.8%) patients received sedation (Fig. 1). Table 1 showed the characteristics of the 2 groups of patients and the comparison results. The mean age (SD) of patients in the no-sedation group was 60.2 (9.8) years, older than the sedation group which was 58.7 (8.7) years (P < 0.001). There was a higher proportion of male in the no-sedation group than sedation group (55.1% vs 50.0%, P < 0.001). 98.8% no-sedation colonoscopies were manipulated in the afternoon. The average withdrawal time was shorter in sedation group (P < 0.001). The reasons for colonoscopy, 77.6% were diagnosis, 19.5% was followed by screening in no-sedation group, and compared with sedation group, 67.2% and 9.6% respectively. The group of sedation colonoscopy have a greater rate of treatment towards polyp.
3.2 Outcomes
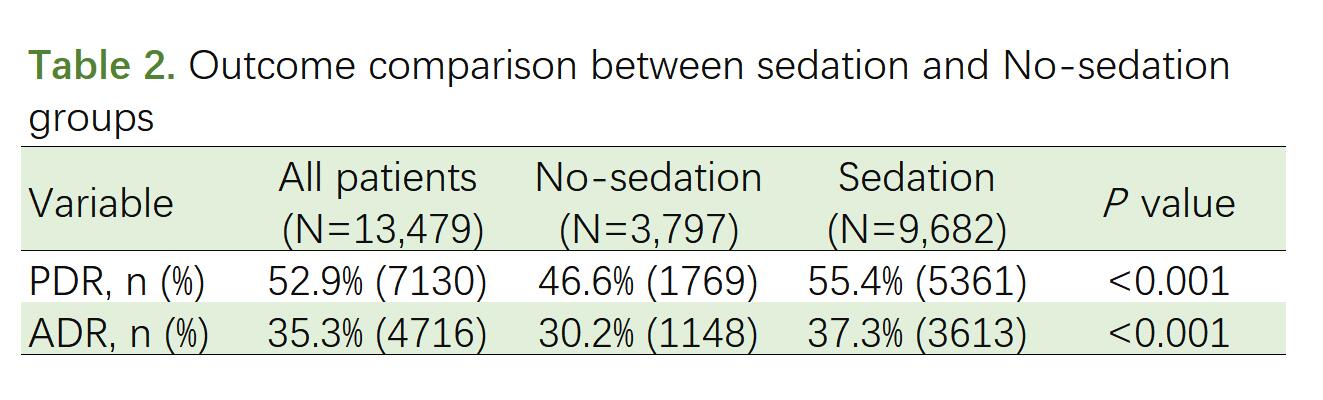
Both PDR and ADR were higher in group with sedation (PDR: 55.4% vs 46.6%, P < 0.001; ADR: 37.3% vs 30.2%, P < 0.001). (Table 2)
3.3 The Effect of Sedation and Interaction Effects between Sedation and Other Factors
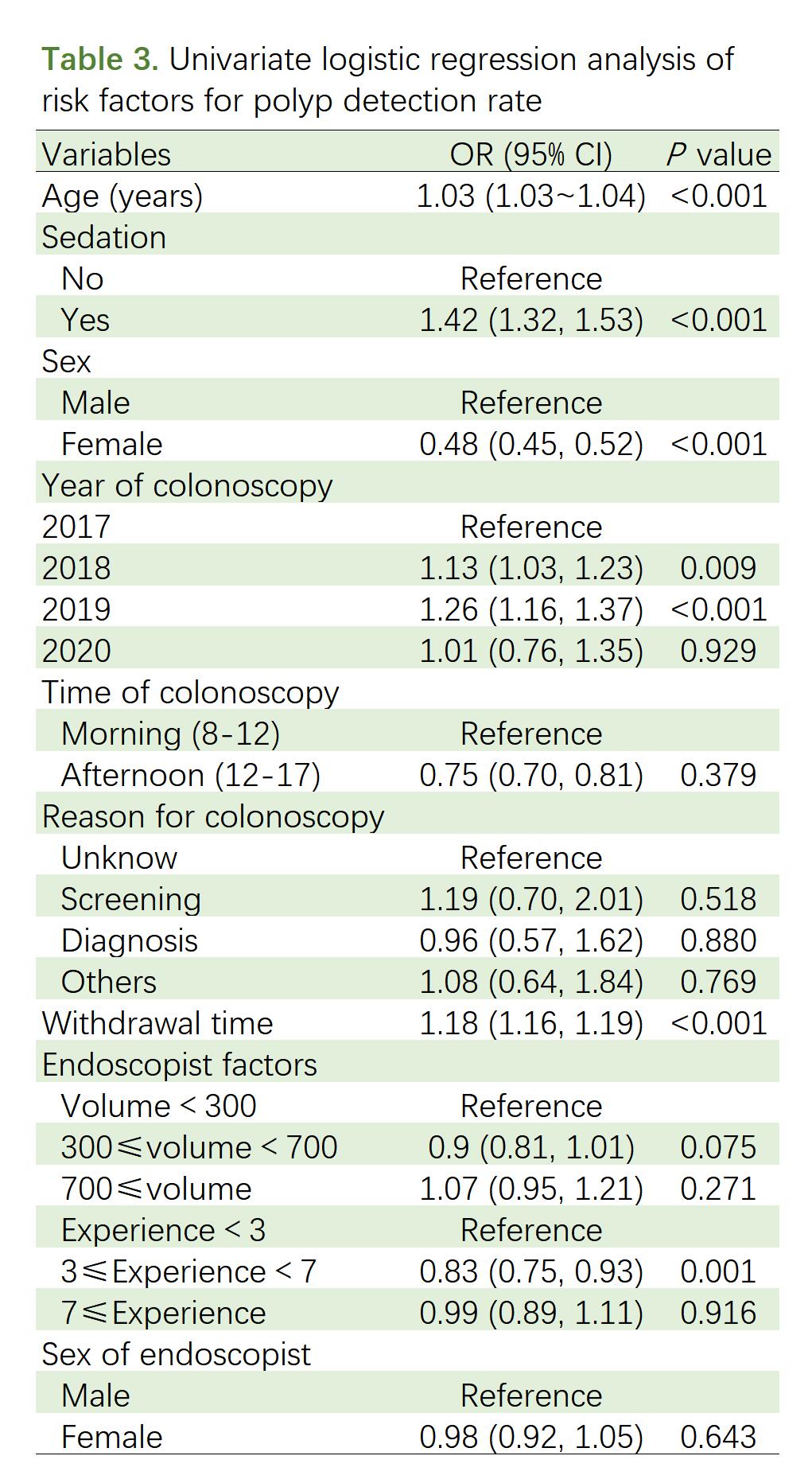
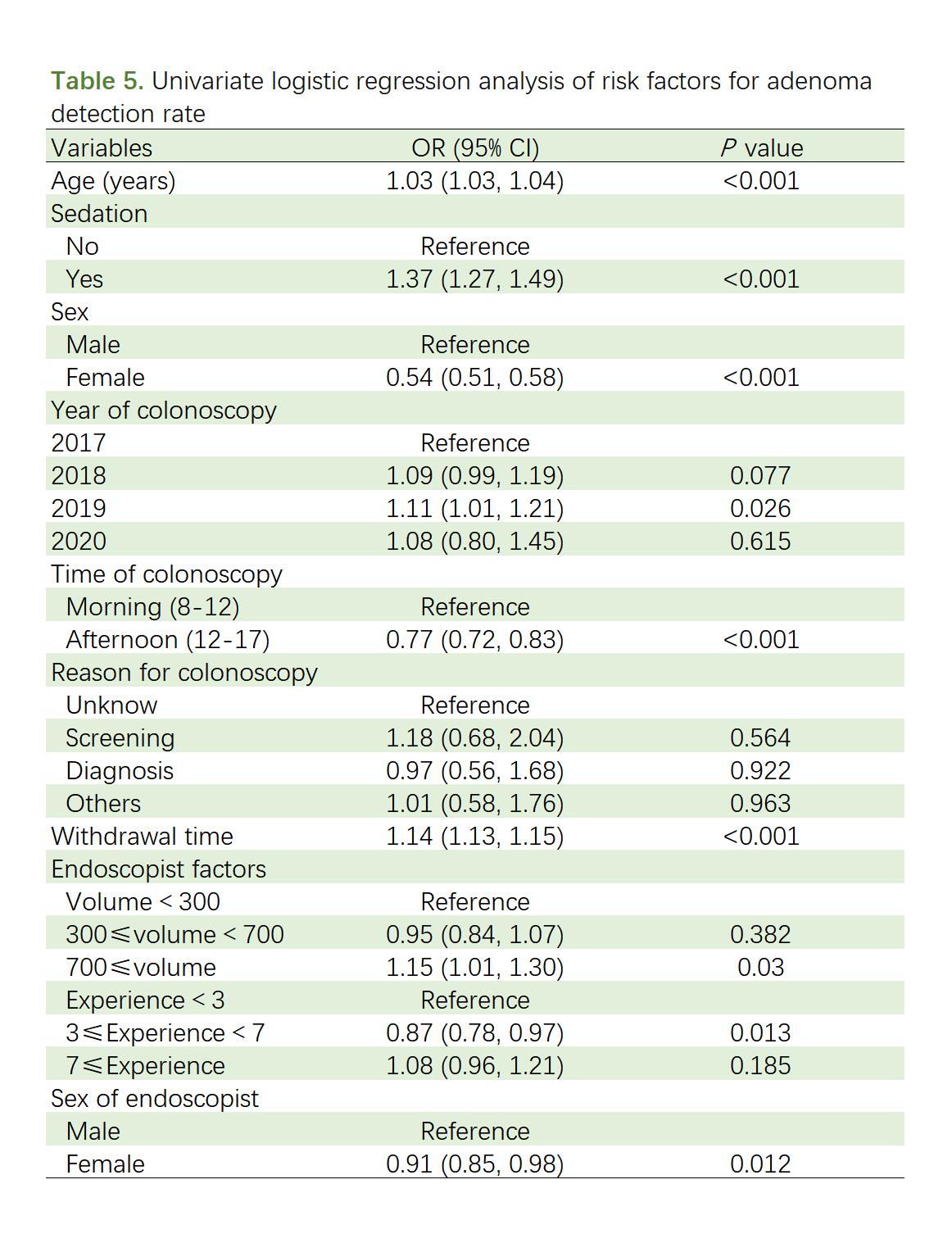
To explore the effect of the factors on the PDR and ADR of the colonoscopy, univariate and multivariate logistic regression analysis were performed. In univariate logistic regression analysis, for patient-level factor, we found that the female patients(OR = 0.48, 95% CI: 0.45–0.52) were negatively associated, whereas age (OR = 1.03, 95% CI: 1.03–1.04), Sedation(OR = 1.42, 95% CI: 1.32–1.53), Withdrawal time (OR = 1.18, 95% CI: 1.16–1.19) were positively associated with PDR. Similarly, the female patients(OR = 0.54, 95% CI: 0.51–0.58) were negatively associated, whereas age (OR = 1.03, 95% CI: 1.03–1.04), sedation(OR = 1.37, 95% CI: 1.27–1.49), withdrawal time (OR = 1.14, 95% CI: 1.13–1.15) were positively associated with ADR. (Tables 3,5).
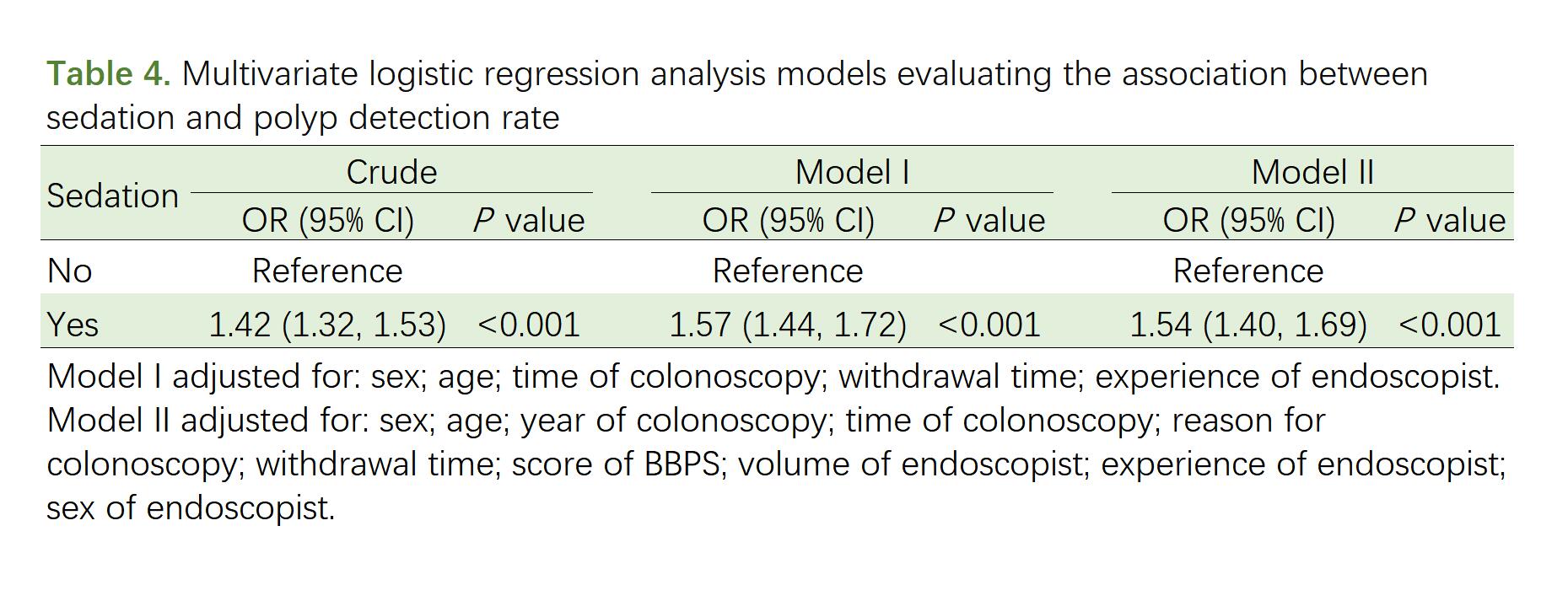
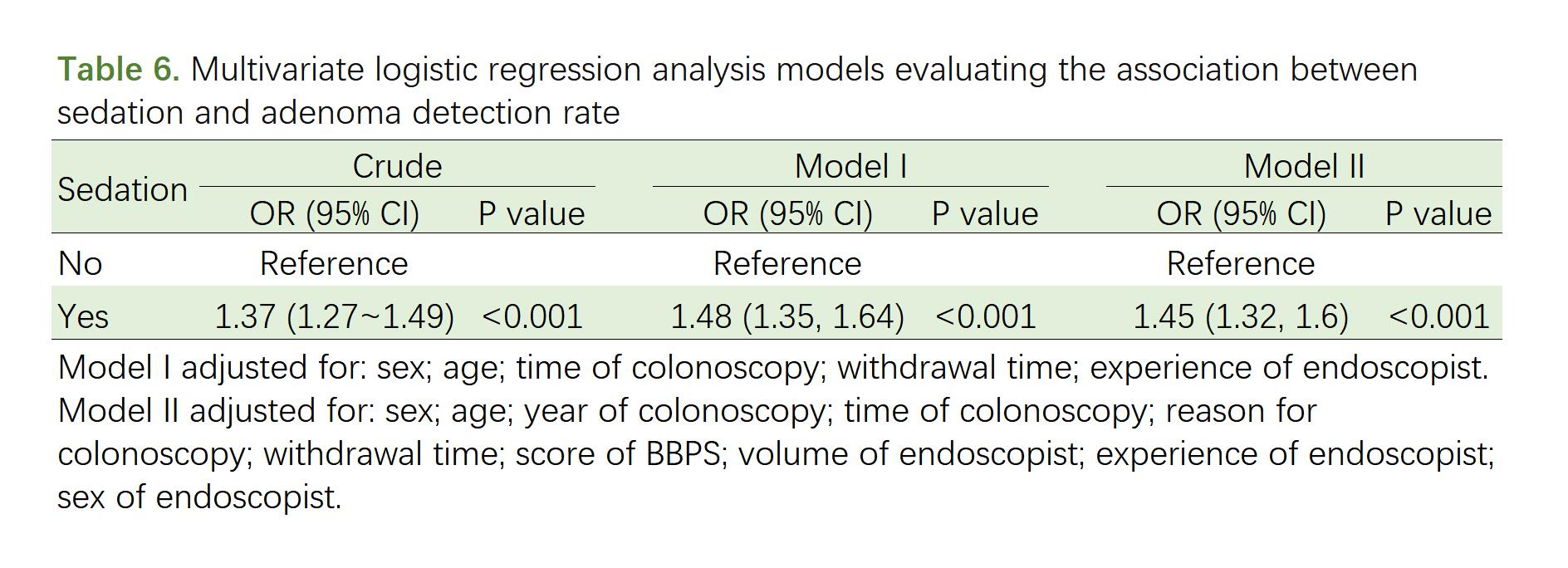
Furthermore, for multivariate analyses, we had constructed regression analysis models including crude, Model I included the factors were statistically significant and Mode II included all factors we collected. After adjusting for sex, age, time of colonoscopy, withdrawal time and experience of endoscopist in Model I and all potential confounders in Model II, the association between sedation and ADR and PDR were still stable in both models[Model I: PDR (OR: 1.57, 95% CI: 1.44 ~ 1.72, P < 0.001) and ADR (OR: 1.48, 95% CI: 1.35 ~ 1.64, P < 0.001) ;Model II: PDR (OR: 1.54, 95% CI: 1.40 ~ 1.69, P < 0.001) and ADR (OR: 1.45, 95% CI: 1.32 ~ 1.60, P < 0.001)](Tables 4, 6).
3.4 Subgroup and sensitivity analysis
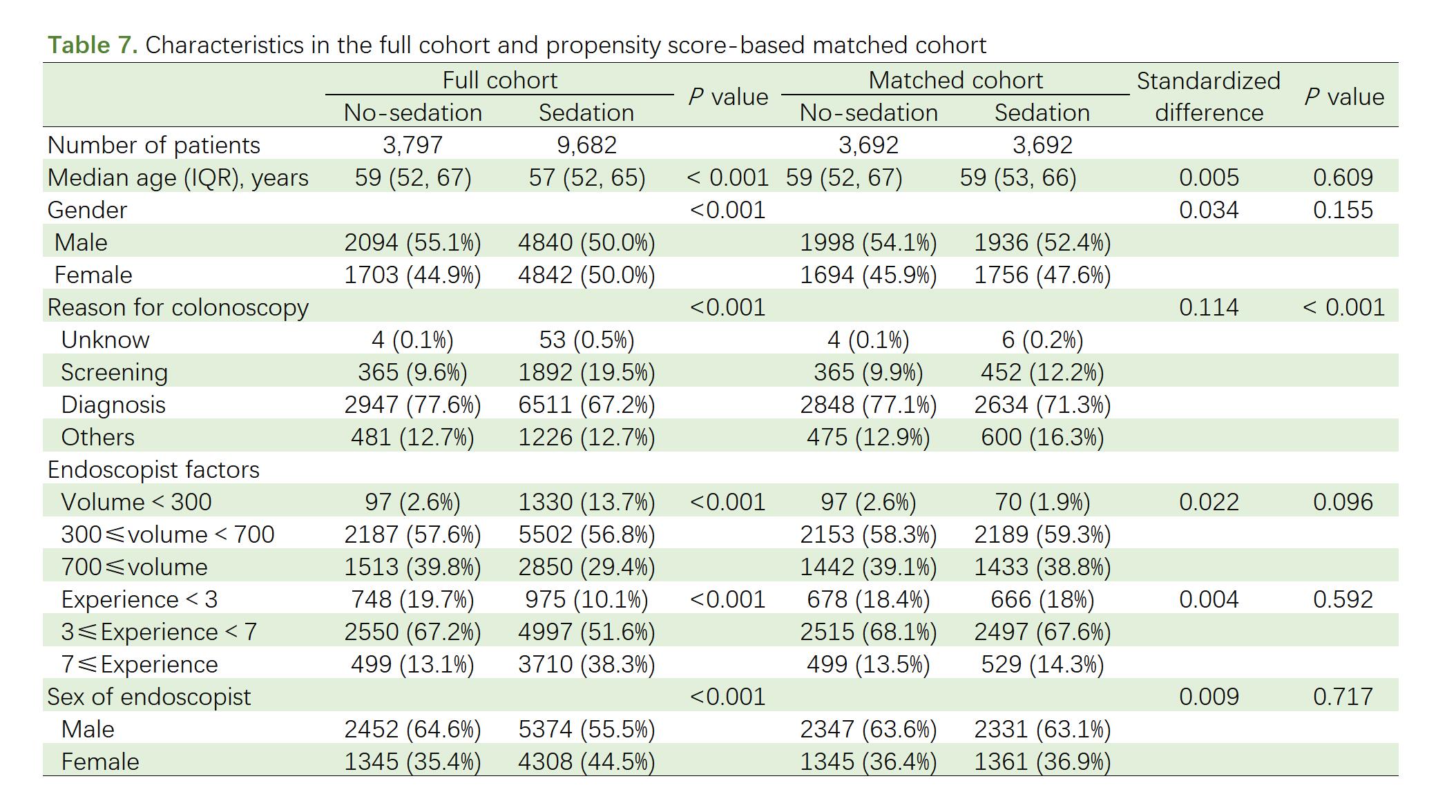
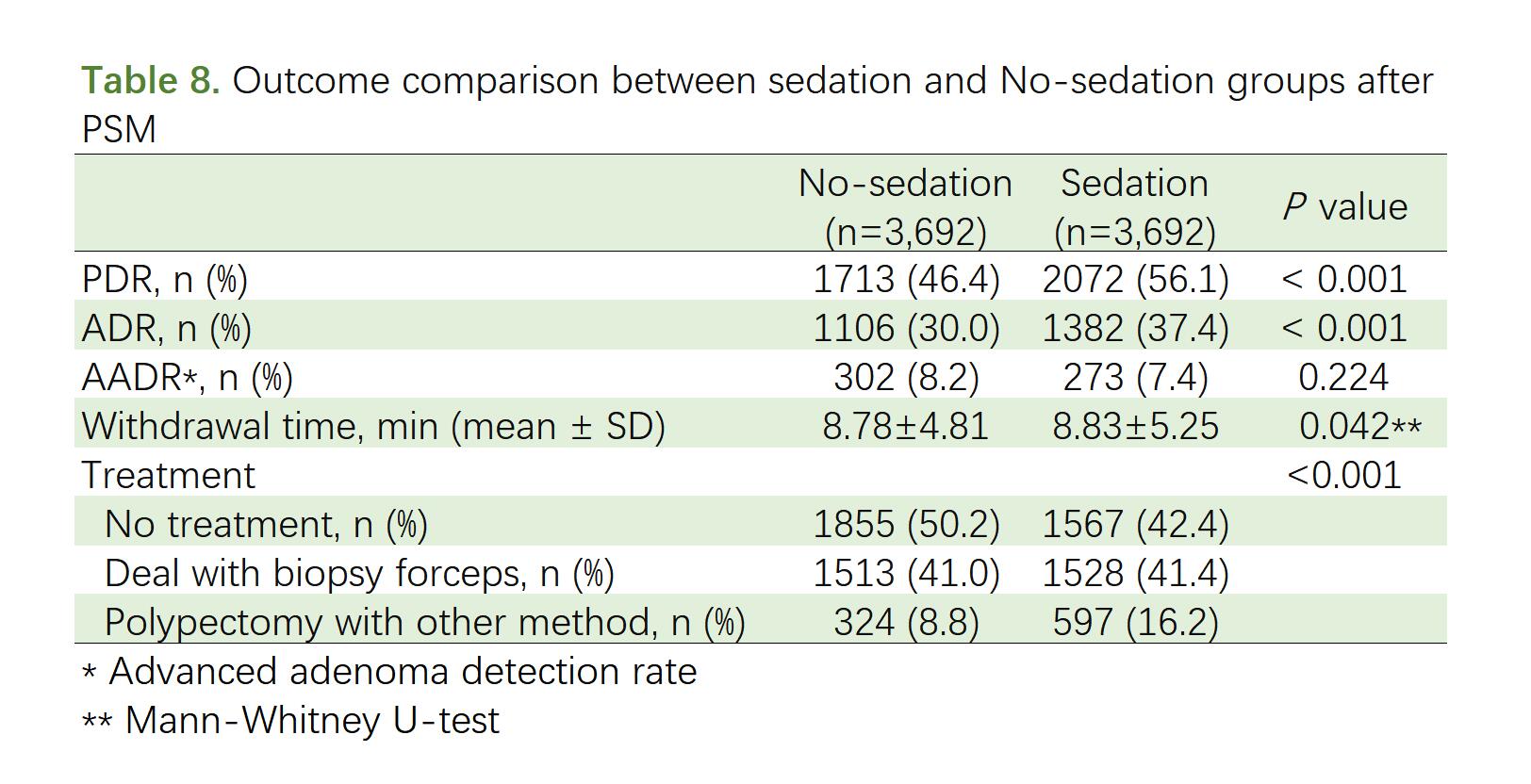
In the subgroup analysis, there was no apparent interaction between any subgroup (Fig. 2 and Fig. 3). After PS matching, the baseline was well balanced between groups except for withdrawal time which was higher in the sedation group (8.83 vs 8.78 minutes, P = 0.042). The PDR and ADR were higher in the sedation group while withdrawal time was longer than in no-sedation group (PDR: 56.1% vs 46.4%, OR: 1.48, 95% CI: 1.35 ~ 1.62, P < 0.001; ADR: 37.4% vs 30.0%, OR: 1.40, 95% CI: 1.27 ~ 1.54, P < 0.001). Comparison between sedation and No-sedation groups after PSM showed that no significant difference was found on detection rate of advanced adenoma (8.2% vs 7.4%, P = 0.224). (Table 8).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}