Search results
Based on the electronic search protocol, a total of 470 studies were initially identified. of these studies, 338 did not meet the inclusion criteria and were therefore excluded. Among the remaining 132 studies, a total of 22 trials met the inclusion criteria[16-37]. Of these 22 included trials, six trials were update reports of published trials[17, 25, 26, 28, 29, 33], one trial involving gastric or GEJ carcinoma[18]. Thus finally 15 randomized controlled trials were included in this meta-analysis (figure 1). Table 1 listed the baseline characteristics of patients and studies. The quality of each included study was roughly assessed according to Jadad scale, four trials[16, 21, 34, 37] were double-blind, placebo-controlled trials, thus had a Jadad score of 5, and the remaining eleven trials were open-label controlled trials, thus had a Jadad score of 3.
Incidence of LVEF decline
A total of 7,184 patients receiving dual HER-2 blockade in 15 RCTs were available for LVEF decline analysis. There were 302 LVEF decline events among these patients. The highest incidence (8.7%; 95% CI 5.3% to 13.9%) was observed in a phase III breast cancer neoadjuvant trial of trastuzumab plus lapatinib when concomitant with paclitaxel [22], while the lowest incidence was observed in four trials in which no events of LVEF decline occurred[16, 27, 31, 37]. Using a random-effects model (χ2-based Q statistic test: Q= 31.75; p=0.004; I2 = 55%), the summary incidence of LVEF decline in cancer patients treated with dual HER2 blockade was 4.6% (95% CI, 3.7% to 5.7%, figure 2A).
For LVEF decline associated with anti-HER2 monotherapy, the highest incidence (13.4%; 95% CI 10.2% to 17.4%) was observed in NSABP protocol B-41 trial[30], while no events of LVEF decline occurred in three trials[16, 19, 37]. Using a random-effects model (χ2-based Q statistic test: Q=108.33; p<0.001; I2=86%), the summary incidence of LVEF decline in cancer patients treated with anti-HER2 monotherapy was 3.2% (95% CI, 2.2% to 4.6%, figure 2B).
Incidence of CHF
A total of 6,818 patients receiving dual HER-2 blockade in 14 RCTs were available for CHF analysis. There were 56 total CHF events among these patients. The highest incidence (2.0%; 95% CI 0.7 to 6.1%) was observed in a phase III breast cancer trial of trastuzumab plus lapatinib after prior trastuzumab-based therapies[33], while no events of CHF occurred in five trials. Using a fixed-effects model (χ2-based Q statistic test: Q=8.26; p=0.82; I2 =0%), the summary incidence of CHF in cancer patients treated with dual HER2 blockade was 0.9% (95% CI, 0.7% to 1.2%, figure 2C). As for CHF associated with anti-HER2 monotherapy, a total of 9,283 patients were included for analysis. Using a random-effects model (χ2-based Q statistic test: Q=52.77; p<0.001; I2 =73.42%), the summary incidence of CHF in cancer patients treated with anti- HER2 monotherapy was 0.7% (95% CI, 0.4% to 1.3%, figure 2D).
Risk of LVEF decline and CHF associated with dual HER2 blockade
All of the 15 included trials reported the LVEF decline data, thus included for calculating the OR of LVEF decline associated with dual HER2 blockade. A total of 284 LVEF decline events were observed in dual HER2 blockade versus 357 LVEF decline events in anti-HER2 monotherapy. The pooled results demonstrated that the dual HER-2 blockade in cancer patients significantly increased the risk of developing LVEF decline with an OR of 1.20 (95% CI 1.02–1.41, p=0.031, Figure 3A) using a fixed-effects model (χ2-based Q statistic test: Q=22.58; p=0.091, I2 =32.6).
A total of 14 randomized trials reported CHF data. A total of 55 CHF events were observed in dual HER2 blockade versus 57 CHF events in anti-HER2 monotherapy. The pooled results showed that the dual HER-2 blockade in cancer patients significantly increased risk of developing CHF with an OR of 1.45 (95% CI 1.00–2.11, p=0.049, Figure 3B) using a fixed-effects model (χ2-based Q statistic test: Q=12.67; p=0.53, I2 =0).
Sensitivity analysis
Sensitivity analyses using Mantel Haenszel or Inverse Variance model showed that the risk of LVEF decline with dual HER-2 blockade was 1.19(95%CI: 1.02-1.41, p=0.031) and 1.18 (95%CI: 1.01-1.40, p=0.041). Similarly, sensitivity analyses using Mantel Haenszel or Inverse Variance model showed that the risk of CHF associated with dual HER-2 blockade was 1.48 (95%CI: 1.01-2.16, p=0.045) and 1.55(95%CI: 1.04-2.25, p=0.032) (supplemental table 1) when compared to anti-HER2 monotherapy.
Sub-group analysis
Firstly, we carried out a subgroup risk analysis stratified according to treatment settings. Our results demonstrated that risk of LVEF decline and CHF was comparable between dual HER-2 blockade and anti-HER2 monotherapy in neoadjuvant or metastatic setting (both p>0.05, table 2). However, the addition of dual HER2 blockade to adjuvant treatment in breast cancer significantly increased the risk of developing CHF (OR 2.00, 95%CI: 1.23-3.24, p=0.005) and LVEF decline (OR1.17, 95%CI: 1.00-1.38, p=0.048, table 2).
The concomitant treatment with anti-HER-2 therapy might impact the ORs of cardiac toxicities. Our combined results demonstrated that concomitant hormonal therapy with dual HER2 blockade in breast cancer significantly increased risk of developing LVEF decline in comparison with hormonal therapy plus anti-HER2 monotherapy (OR 4.51, 95%CI:1.24-16.40, p=0.022), while no concomitant treatment or concomitant chemotherapy with dual HER-2 blockade did not increase the risk of developing LVEF decline(p=0.19 and p=0.11, respectively). As for CHF events, concomitant chemotherapy with dual HER2 blockade treatment significantly increased the risk of developing CHF when compared to anti-HER2 monotherapy plus chemotherapy (OR 1.47, 95%CI: 1.00-2.16, p=0.052), while no concomitant treatment or concomitant hormonal therapy with dual HER-2 blockade did not increase the risk of CHF (p=0.22 and p=0.59, respectively).
We also did sub-group analysis according to anti-HER-2 monotherapy. Our result showed that dual HER-2 blockade significantly increased the risk of developing LVEF decline (OR 1.49, 95%CI: 1.14-1.96, p=0.004) when compared to lapatinib, but not for CHF (OR 2.62, 95%CI: 0.90-2.94, p=0.11). In comparison with trastuzumab alone, no significantly increased risk of developing LVEF decline(p=0.37) and CHF (p=0.24, table 2) was observed in dual HER-2 blockade group.
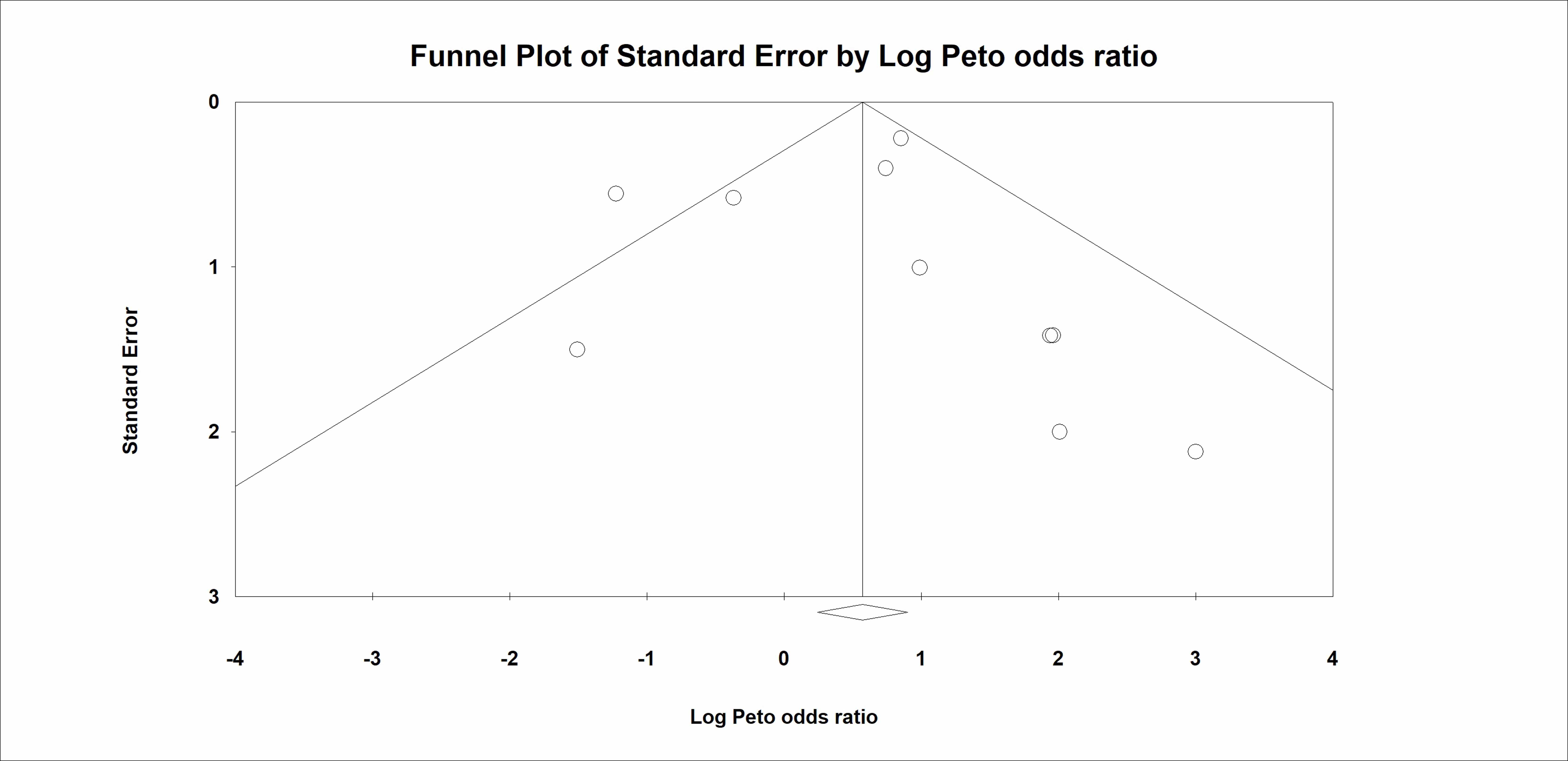
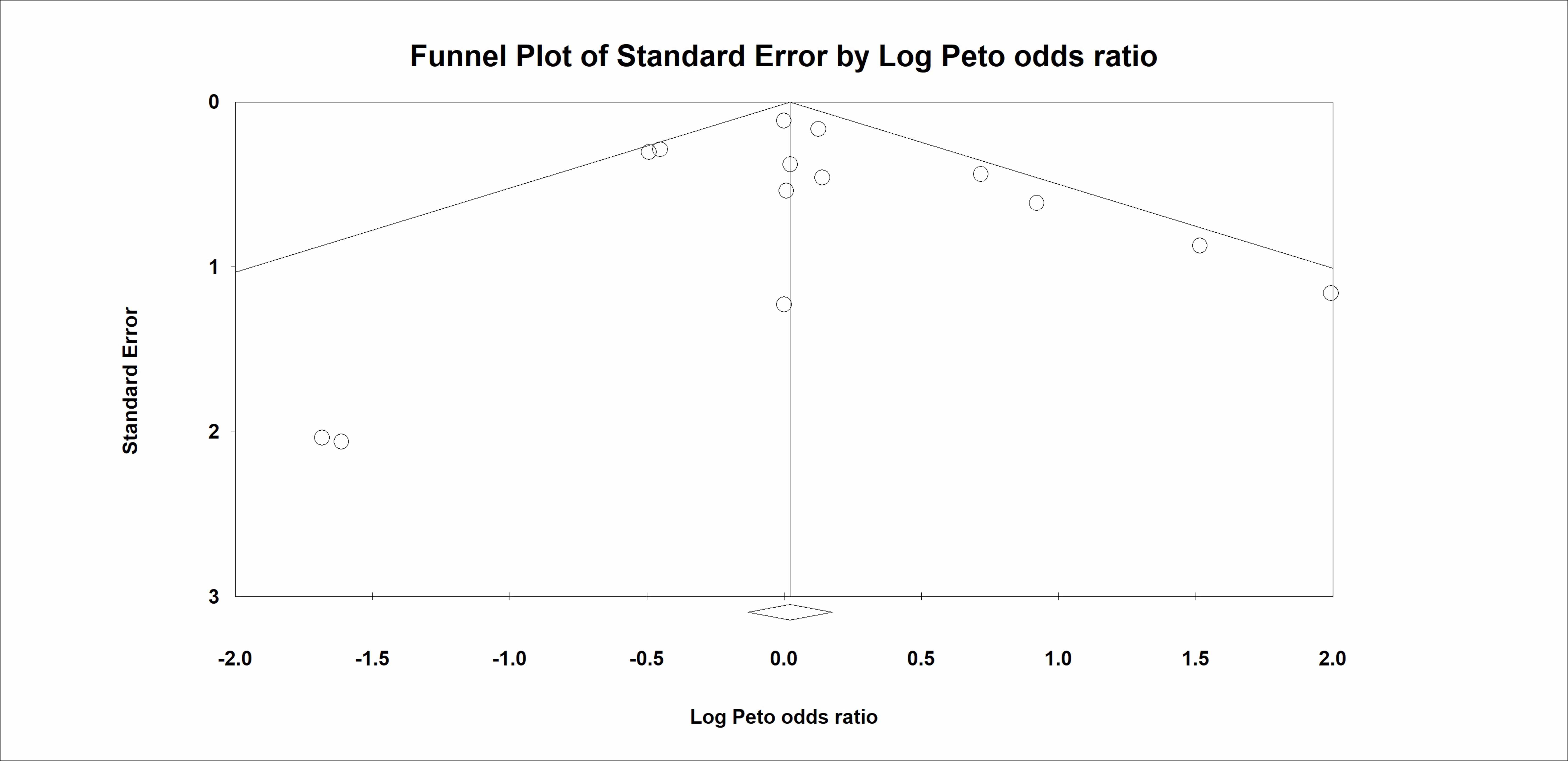
Publication Bias
We performed Begg’s funnel plot and Egger’s test to detect the publication bias of literatures. No significant evidence of publication bias for LVEF decline and CHF was detected by using funnel plots (supplemental figure 1 for LVEF decline; and supplemental figure 2 for CHF), Begg’s test (LVEF decline, p=0.62; CHF, p=0.53) and Egger’s test (LVEF decline, p=0.38; CHF, p=0.93).
{kind=link}
{kind=link}