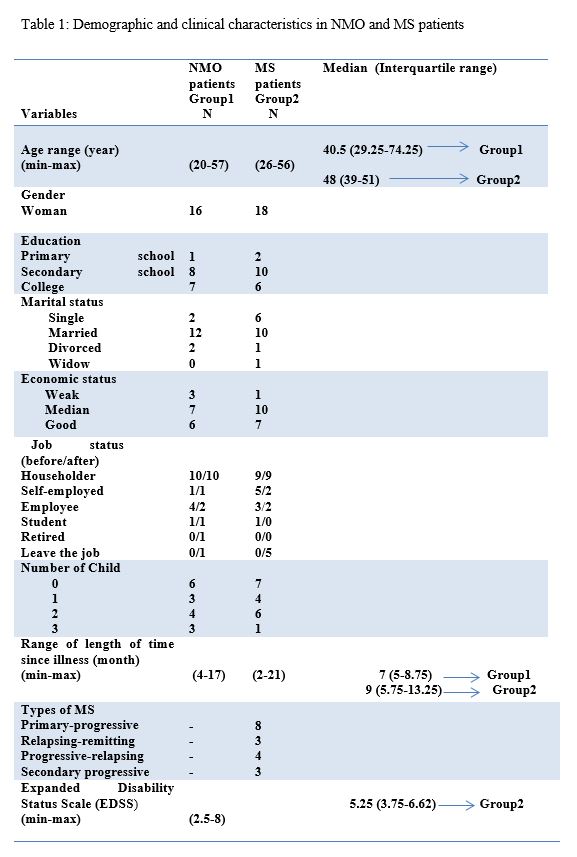
The mean age (SD) of the participants was 39.13 ± 11.14 years in the NMOSD group and 44.83 ± 8.76 years in the MS group. Most of the women in both groups were married, and half of the women in both groups lived in Tehran. The majority of the patients had a bachelor's degree in the NMOSD group and a high-school diploma in the MS group. The mean (SD) duration of NMOSD was 8 ± 3.98 years and the mean duration of MS was 9.55 ± 5.11 years. Table 1 lists all the characteristics of the two groups.
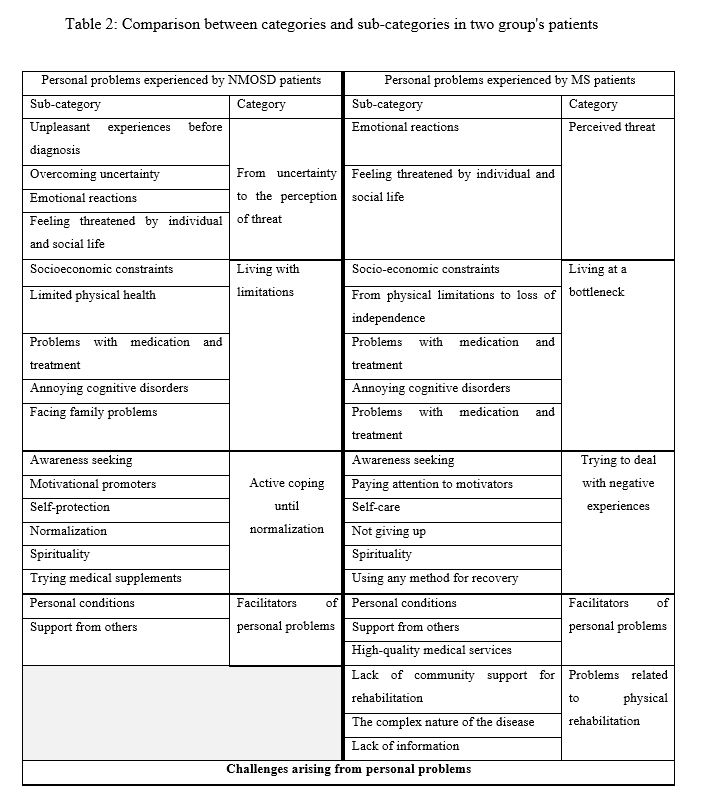
A common theme for both groups was the "challenges of personal problems". The categories were named after each other and had many similarities. The categories belonging to the NMOSD group were grouped under four categories: "from uncertainty to the perception of threat", "living with limitations", "active coping until normalization", and "facilitators of personal problems". In patients with MS, five categories emerged: "perceived threat", "living at a bottleneck", "trying to cope with negative experiences", "facilitators of personal problems", and "problems related to physical rehabilitation" (Table 2).
The first category in the NMOSD group and MS group was, respectively, "from uncertainty to the perception of threat" and "perceived threat". The majority of NMOSD patients stated that they had suffered a lot before being diagnosed with the disease, and had experienced many problems due to lack of diagnosis:
"Both my doctor and my family thought I had a mental illness and could not believe my eye problems and pain. I even went to a psychologist and, because of my late diagnosis, my illness progressed." (NMOSD patient #2)
Most NMOSD patients were happy with the diagnosis. However, MS patients talked less about the complexity of diagnosing the disease and more about the fatigue caused by the disease before diagnosis. These people usually lived in remote cities that did not have access to magnetic resonance imaging (MRI). Most of the MS patients experienced a gradual onset and continuous progression of signs and symptoms without any recurrence:
"I had MS for a while and I didn't know it. The first time I went to the doctor, I told him the problems I had. He said, 'You only have a stomach problem.' Our city did not have MRI equipment, or a good doctor. First I got weaker. I went to Kermanshah [the center of Kermanshah Province]. The first doctor I visited ordered an MRI. Then, he said, 'You have MS.'" (MS patient #7)
The sub-category of "emotional reactions" was common to both groups and included crying, sadness, grief, and anger. The sub-category "feeling threatened by individual and social life" was also common to both groups:
"I was worried I might not be able to get married because of MS." (MS patient #8)
"Living with limitations" and "Living at a bottleneck" were two similar categories in NMOSD and MS patients, but had slightly different sub-categories. In NMOSD and MS patients, social and economic constraints included exposure to harassment from others, isolation, changes in work and education, and the financial pressures of the treatment. Examples are given below.
Drug-related problems in NMOSD and MS patients included a shortage of medicine and the high price of medicine. One of the patients said:
"Our medicine is very expensive. I spent about 9 million rials on one medication, and this put me under financial pressure." (MS patient, #7)
Limited physical health in NMOSD was another sub-category that included items such as feelings of overwork and fluctuating dependence on others; reduced housework, leisure, and activity; quitting sports; and reduced sex.
"I am not as active as I used to be, and I go out less. I don't go to the gym because I may fall down. When I'm entertaining a guest and because my hand goes numb, I spill hot tea and burn my hand..." (NMOSD patient #14)
Annoying cognitive disorders was another sub-category. Many patients with MS and NMOSD reported cognitive impairment. Similar to NMOSD patients, MS patients suffered from memory impairment:
"Sometimes I forget that I have to go to work in the morning, and they remind me." (MS patient #15)
NMOSD and MS patients also faced family problems:
"When my husband found out that I was sick, he said that the cost of treatment and medicine was high and that he couldn't pay it, and so we got divorced." (NMOSD patient #16)
Another category was "from active coping until normalization", which emerged in the NMOSD group. There were similarities and differences between the two groups in the subgroups described below.
Awareness seeking was common between the two groups. The NMOSD patients had no knowledge of their disease when they heard the word NMOSD, and some called it pseudo-MS. With the help of Internet searches and asking doctors and nurses, they managed to obtain more information. Patients with MS, like patients in the NMOSD group, sought information and even used the radio and television to complete their information.
"As soon as the doctor said that I have NMOSD, I began searching the Internet to see what the disease was, what made it better, and what made it worse." (NMOSD patient, #3)
Motivational promoters were another sub-category in both groups. Patients tried to motivate themselves by considering worse conditions and by paying attention to motivation enhancers.
People tried not to lose hope in various ways and sought to find motivation to continue living. Some had tried to give themselves hope and motivation by continuing to exercise, learn more, compare themselves to unsuccessful cases, or successful role models and improved patients.
"I felt hopeful to see that people who used to sit in wheelchairs could now walk. I thought they could never walk after the attack." (MS patient #8)
Participants protected themselves by seeing a doctor, by avoiding stress, negative thoughts and people, and having more rest. The following codes emerged: "self-preservation" sub-category in NMOSD patients, but "self-care" in MS patients. Loss of energy and fatigue made MS patients learn energy conservation techniques, so codes such as activity planning, lifestyle changes (elimination of bad habits, improvement of eating patterns), adaptation of the environment, and exercise resulted in the self-care subcategory.
"I had a lot of wrong habits; I quite everything to keep my energy and stay healthy. For example, I stopped taking a shower with hot water or did many exercises to improve my physical condition." (MS patient, #7)
Normalization was another sub-category. The participants talked about being indifferent to the disease, getting used to the pain, normalizing, understanding the disease, not taking the disease seriously, not having negative thoughts, and equating themselves with healthy people. However, MS patient tried to gain self-confidence and preserve their independence. Hence, "do not give up" emerged from the codes.
"I tried to increase my self-confidence by ignoring my disabilities and paying attention to my abilities, so that I would not get lost." (MS patient, #4)
"I no longer feel sick at all; I got used to it. I even take care of my leg." (NMOSD patient, #5)
Spirituality was in common between the two groups. The majority of participants found a deeper connection to God following the illness. Prayer, trust, and appealing to the Imams (saints) were the themes that formed the sub-category of spirituality.
"At first, it was as if something had happened to me. I was constantly praying, and I didn't even listen to music." (NMOSD patient, #12)
"Trying medical supplements" and "using any method for recovery" were two sub-categories that were similar for NMOSD and MS patients. The only difference was that patients with MS used more methods to improve their body, e.g., turning to traditional medicine, acupuncture, and bee therapy.
"My husband took me to a friend, and he said that if I tried bee treatment, I'd feel better. But it didn't work at all." (MS patient, code 9)
The category "facilitators of personal problems" emerged in both groups of patients. In the NMOSD group, this category included personal conditions (i.e., marriage, family support, beliefs) and support from others. In the group of MS patients, it included personal conditions, support from others, and access to high-quality medical services. Support from others meant support from people other than the family. Donations from charities, colleagues, friends, and distant relatives were among the contributions mentioned by the participants.
The sub-category of "benefiting from high-quality medical services" in people with MS emerged due to the frequent use of occupational therapy and physiotherapy services by most of these patients.
"My husband helps me a lot, and he is the only one who can calm me down – after God, of course." (MS patient, #17)
Finally, the sub-category of "rehabilitation-related problems" existed only in the group of MS patients and included a) lack of community support for rehabilitation, b) the complex nature of the disease (i.e., recurrent disease, time-consuming diagnosis, young age, and chronicity), and c) lack of information (i.e., family and patient's poor and incomplete information about care, insufficient information about the disease, and inadequate community views.)
It seems that the reason for the existence of this category only for this group of patients is the large number of disabled people, the community's little information about disability, and lack of equipment for the disabled, lack of government support for patients in accessing care services, absence of insurance services, and unsafe streets.
"There is no one to follow me up and check why I couldn't come for treatment. Also, MS treatment centers are small and far away." (MS patient, #8)
{kind=link}
{kind=link}