The existence of TSH receptor antibody and the change of its titers have important clinical significance for diagnosis, treatment and prognosis evaluation of GD. American Thyroid Association (ATA) guidelines suggest that, in patients with hyperthyroidism, especially when there are no typical signs of diffuse thyroid enlargement or orbitopathy, positive TRAb is a simple and effective marker that helps identify GD, with a good cost-benefit ratio (14). Although the third-generation automated TRAb detection has already possessed high sensitivity and specificity, it cannot distinguish the types of stimulating or inhibitory antibodies. In contrast, bioassays based on measuring increased cyclic AMP production in cellular systems can specifically detect the levels of TSI, but it limited in laboratories due to fussy and time-consuming steps. In recent years, a new automated TSI assay, using a pair of recombinant human TSH receptor in a bridging format to capture and detect thyroid-stimulating autoantibodies, has been developed and reached in the market of China [9]. Here we evaluated the clinical performance of this new automated TSI immunoassay in comparison with third generation TRAb assay.
In this study, we recruited participants with hyperthyroidism, Hashimoto's thyroiditis, non-autoimmune thyroid diseases and non-thyroid diseases, covering the spectrum of common outpatients. Quantitative analysis showed that the bioassays of Immulite 2000 TSI and Roche TRAb had a relatively high correlation (with a slope of 0.999) and excellent concordance (with a 96.73% overall agreement). According to the cutoff value proposed by the manufacture, the positive rates of TSI and TRAB in new-onset GD patients were 96.92% and 95.15%, respectively, which suggested that the presence of TSH receptor antibody can be used as a key indicator of GD. In line with the results of other studies, the sensitivity and specificity of TSI and TRAb in GD diagnosis were both high and had no significant differences. However, in comparison with TRAb, the qualitative analysis of discordant cases showed that TSI assay is more consistent with the clinical diagnosis of GD.
The correlation between TRAb and TSI and thyroid functions was controversial in previous studies. Kabadi et al. found there was no significant correlation between the levels of FT4 and TSI in a study using bioassay to detect TSI[18]. In the study by Frank et al.[9], TSI showed a more significant correlation with FT4 than compared with TRAb. Here we found both TSI and TRAb levels positively correlated to FT4 and FT3 levels in newly-onset GD patients, which is consistent with the results reported by Allelein et al. [14]. The correlation between the titers of TSI/TRAb detected by different methods and the degree of hyperthyroidism need to be explored in the larger number of GD patients in different populations.
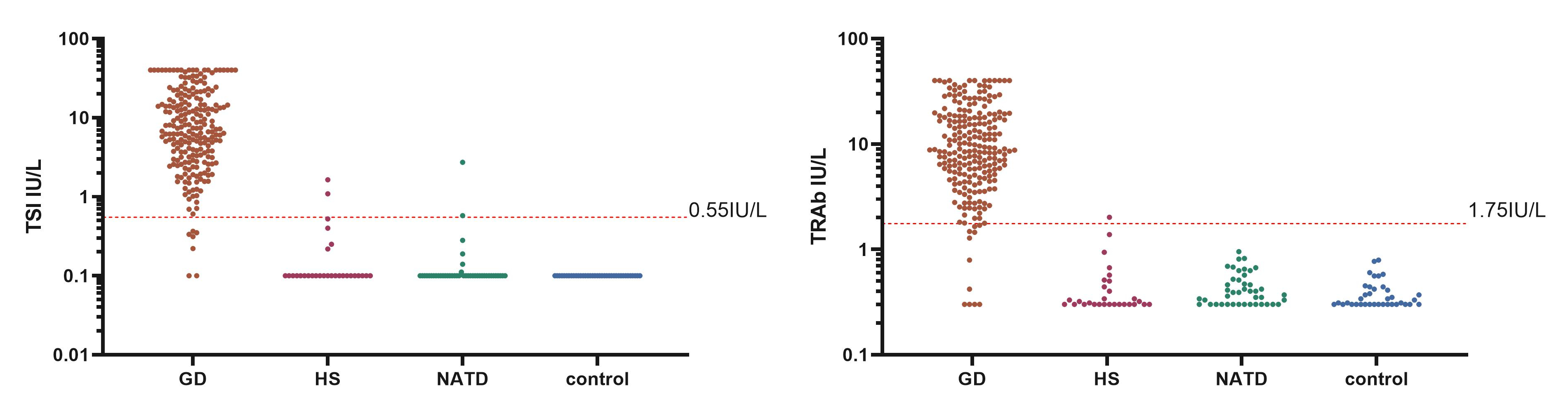
By ROC curve analysis, a new cut-off value of TSI 0.577 IU/L for GD diagnosis was obtained in this study, with the sensitivity of 96.9% and specificity of 97.2%, respectively. This new cut-off value was very close to the cutoff value (0.55IU/L) provided by the manufacturer, as well as new cut-off value reported in several studies (0.54IU/L, 0.57IU/L, 0.55IU/L, respectively) [9, 15, 16]. Correspondingly, a new cut-off value of 1.38 IU/L for TRAb was identified in this study, with the sensitivity of 96.9% and of specificity 99.1%, respectively, which was slightly lower than the cutoff value (1.75IU/L) proposed by the manufacture, but was similar to the cut-off value 1.25 IU/l reported by Tozzoli et al. in an Italy study [19]. If the value of TRAB 1.38IU/L obtained in this study was applied for GD diagnosis, the rate of missed diagnosis would be reduced to a certain extent (Table S3). In short, given that the difference in race, sample size, disease status, GD definition criteria, treatment or not, detection method and the source of the kit, the positive cut-off value of TSH receptor antibody may be different. Achieving uniform detection and discrimination standards is a key move to incorporate autoimmune antibody indicators into the diagnostic criteria.
After the previous study of Immulite 2000 TSI assay in GD diagnosis[10], we reported that an automated commercial TSI kit and the positive cut-off value 0.55IU/L can be used for routine clinical testing of GD in Chinese population. Moreover, the coincidence rate between TSI detection and clinical GD diagnosis was higher than that of TRAb, which suggests that the fully automated TSI assay will have better application value in the differential diagnosis of hyperthyroidism. This study recruited a large sample of newly-onset GD patients, which confirmed the diagnostic efficacy of TSI for GD, but also verified the usability of the cut points provided by the kit. However, this was a single-center cross-sectional study of newly-onset GD patients. Its generality need to be further verified in more studies and larger populations. The application value of TSI indicators in GD outcome and recurrence prediction also need to be evaluated in future studies.
In conclusion, both TSI and TRAb assays had relatively high diagnostic accuracy for GD. The newly-marketed automated TSI detection had a higher coincidence rate with GD clinical diagnosis, and was expected to be popularized in clinical practice.
{kind=link}