Act-D and MTX act through distinct anti-tumor mechanisms and should be compared with regards to efficacy and safety. With the paucity of comprehensive comparisons of therapeutic effectiveness and toxicity for the two drugs as first-line chemotherapy for LRGTN patients, we included 8 RCTs and 9 non-RCTs (1674 patients) in the present meta-analysis. Given that LRGTN patients who like to preserve their fertility would firstly receive single-agent chemotherapies, such as Act-D and MTX, and these agents have several dosing/cycling options, our study regarded all Act-D-based regimens and MTX-based regimens as one entity, respectively [3, 4]. Similar to observations from previous meta-analysis investigating the efficacy of Act-D and MTX [9, 10], our results confirmed that Act-D had greater superiority in terms of complete response than MTX, irrespective of dosage and cycle. Of note, we have obtained some unique findings that some toxicities such as nausea, vomiting, and alopecia are more common in LRGTN patients treated with Act-D-based regimens, and liver toxicities were more commonly associated with MTX-based regimens. However, a previous net-work meta-analysis by Li et al. found that nausea and vomiting were more frequently observed in 5d-IM MTX regimen, which was inconsistent with our results [10]. With a tailored study design in which LRGTN patients diagnosed according to the Hammond criteria were also included, our pair-wise meta-analysis included more studies and patients, and gave more comprehensive comparisons. Accordingly, the present meta-analysis will aid reference centers and patients to select more effective agents and optimize toxicity management for patients with LRGTN.
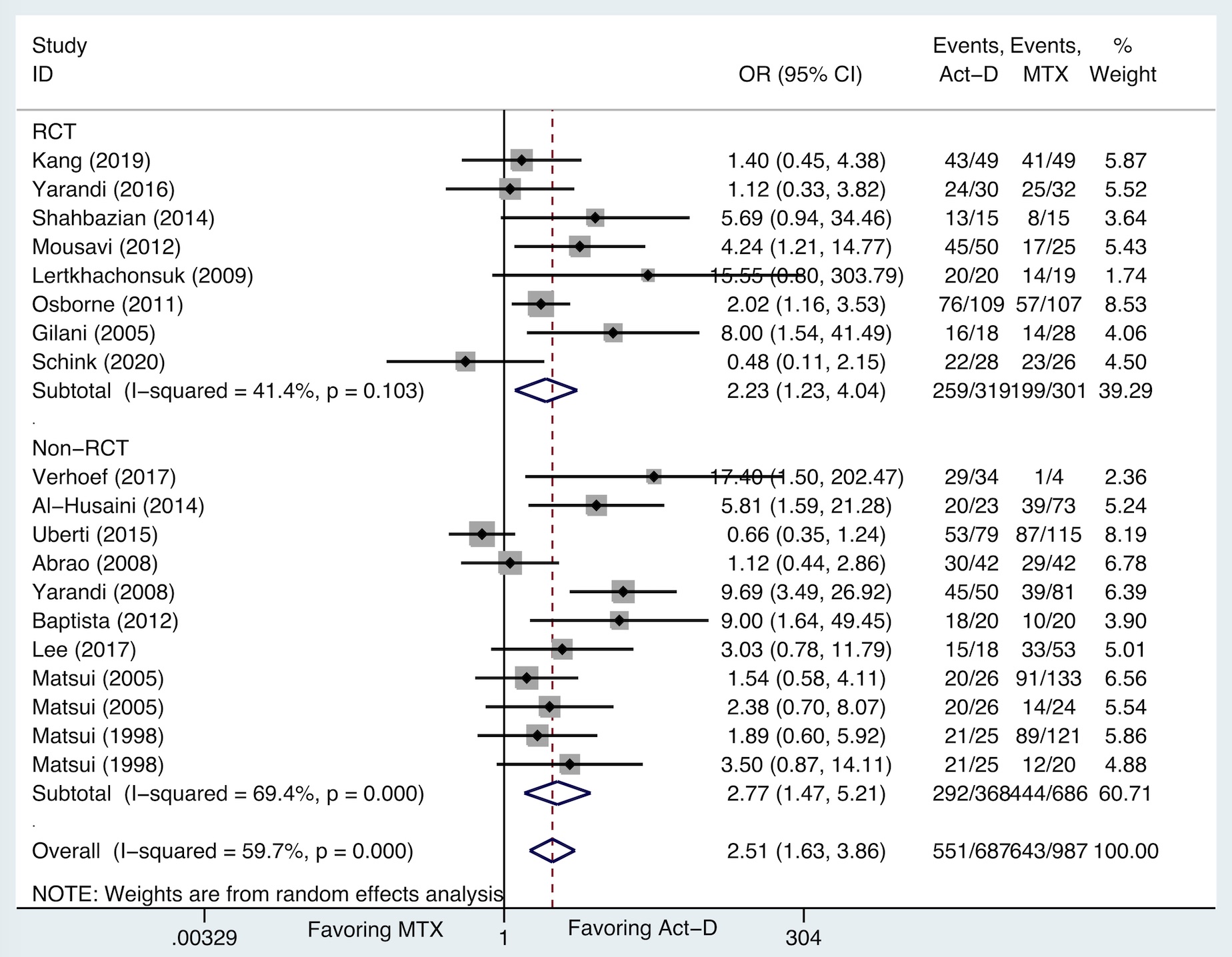
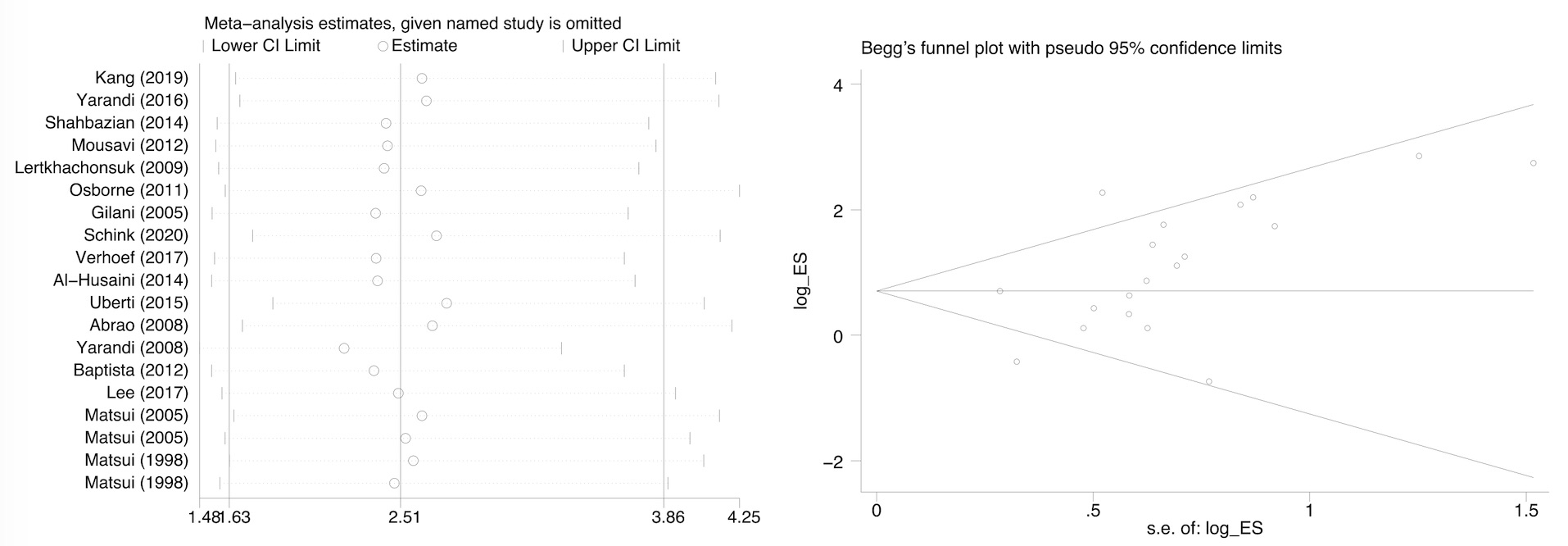
Patients with GTN are now identified as a lucky group that have preferable responses to chemotherapy. The prognosis has significantly improved over the past decades from almost hopeless to a new situation in which the majority of the GTN patients can achieve complete remission, even if a metastatic condition exists. Particularly, LRGTN patients may more likely yield better cure rates to single-agent regimens such as Act-D and MTX, with resulting survival rates approaching 100% [3–5]. Currently, Act-D and MTX have been administered in various regimens with different dosages and cycles, which have been proposed by different reference centers. Although RCTs and retrospective studies have investigated different regimens of Act-D and MTX, there is still no universal consensus on the optimal dosing and cycling for both Act-D and MTX, which was reflected in variability of complete remission rates in different studies. From an overall perspective, our study is an opportunity to move away from comparisons that have centered on specialized regimens, to focus more on the entity instead. The results of our analysis indicated that Act-D-based regimens are more effective than MTX-based regimens as first-line chemotherapy for LRGTN patients. Given the fact that GTN is a rare disease and a limited number of patients are available for randomized clinical studies [35], we included both RCTs and non-RCTs to pool the data. Impressively, stratified analysis showed that pooled OR for complete remission of RCTs was similar to that of non-RCTs, although the quality assessment indicated some methodologic defects of nature for non-RCTs. With this small effort, both randomized trials and nonrandomized or retrospective studies are warranted and should be better orchestrated for LRGTN patients, to not only share valuable clinical experiences but also explore more possibilities of treatment.
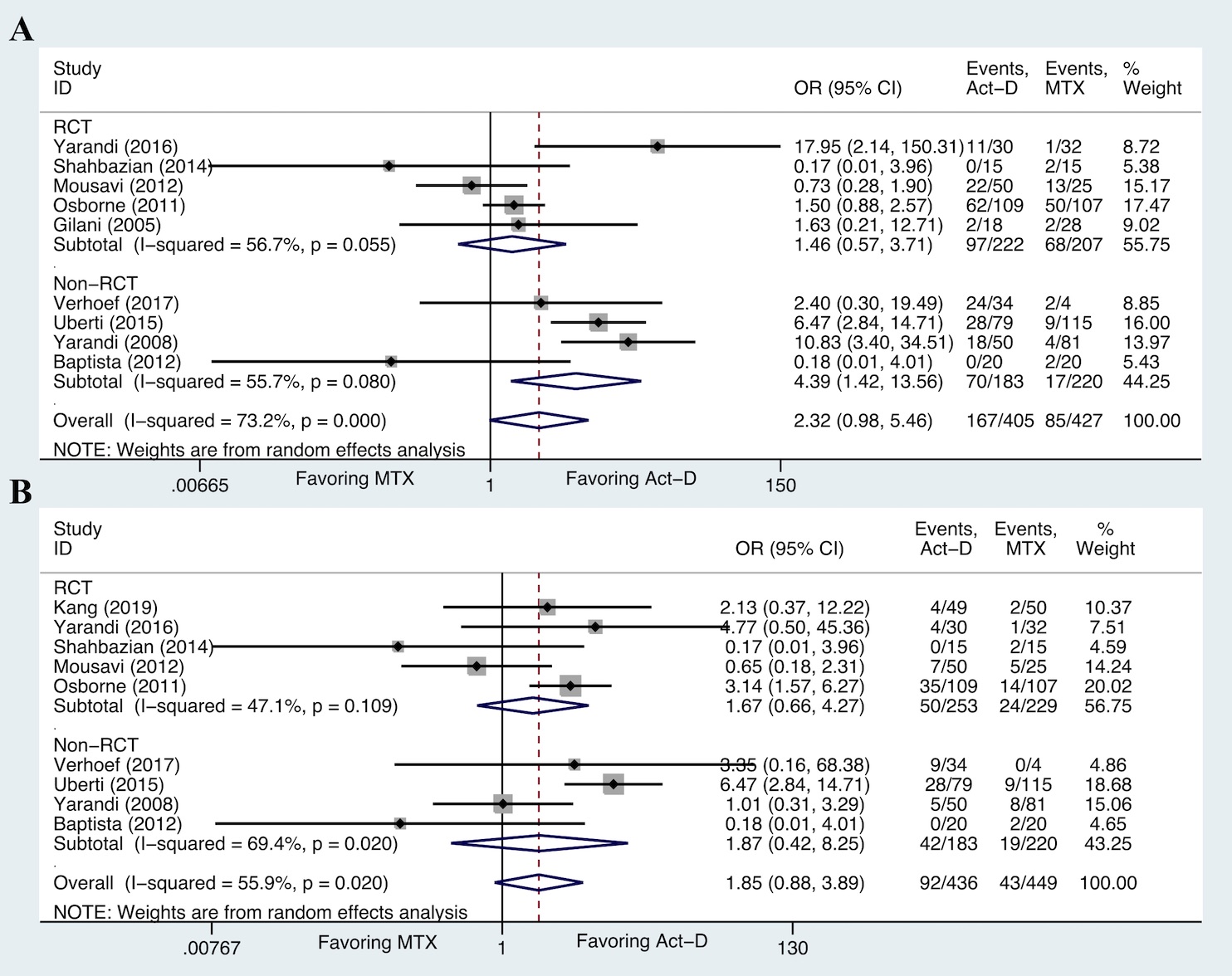
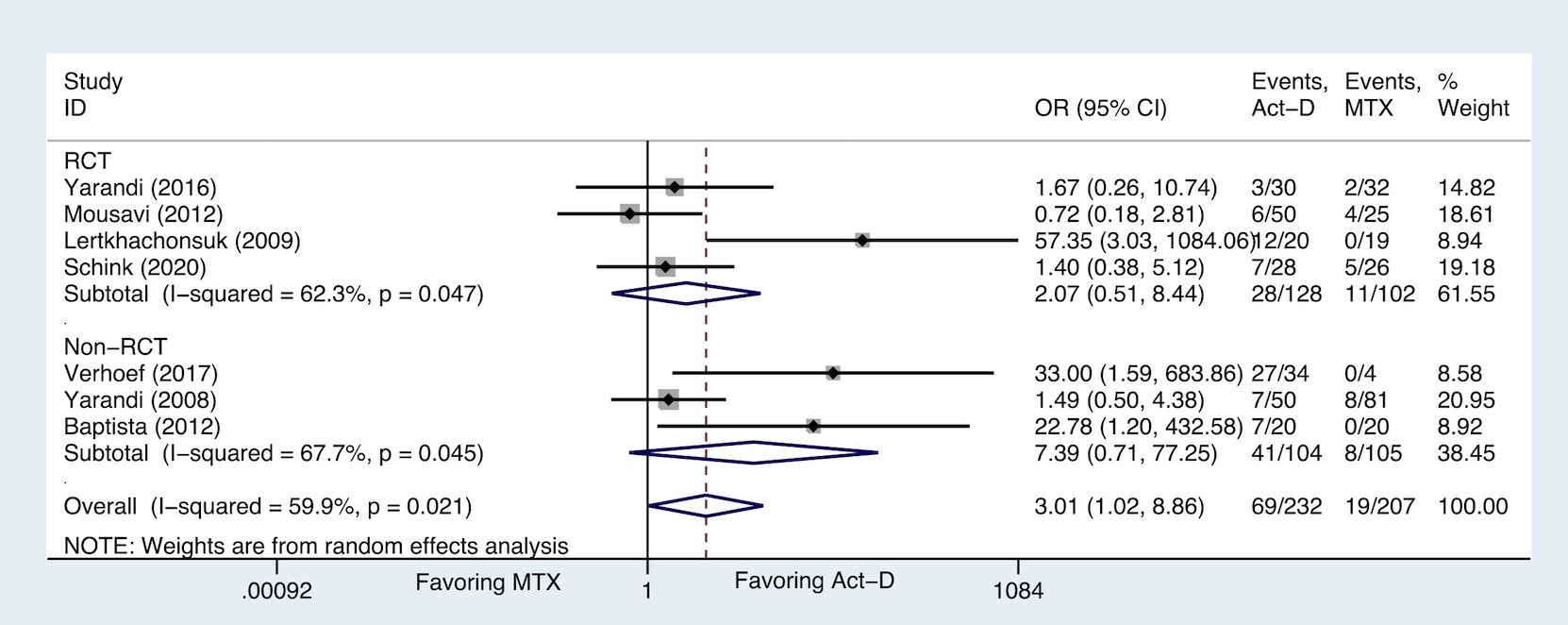
Since the overwhelming majority of LRGTN patients have been able to attain complete remission from first-line single-agent chemotherapy and drug resistances could be successfully salvaged, the ideal drugs and regimens for LRGTN are considered to be minimizing toxicities and maximizing efficacy [34]. Of the toxicities reported in the included studies, a substantial proportion were hematological and gastrointestinal, and the remainder were a mixture that affected other organs. As for hematological toxicities, the forest plots of ORs did not demonstrate differences between Act-D and MTX, but the pooled incidences of anaemia, neutropenia, and thrombocytopenia for Act-D were slightly higher, with the exception of leucocytopenia. Myelosuppression of Act-D was not merely seen in GTN patients. One study found that 39% of the breast cancer patients who had received Act-D chemotherapy suffered mild to moderate myelosuppression [36]. However, Act-D was commonly used for GTN patients and relatively less-used for other tumors, particularly highlighting the importance of managing hematological toxicities in GTN patients. In terms of gastrointestinal toxicities, patients treated with Act-D significantly suffered more nausea and vomiting, which was confirmed by the forest plots and pooled incidences. However, the network meta-analysis by Li et al. suggested that Act-D was less toxic than MTX, although some Act-D-based regimens seemingly lost favor because of nausea and alopecia according to previous studies [37]. In addition, alopecia and anorexia were more frequently seen in patients treated with Act-D, indicating that Act-D may affect skin and nutrition metabolism. Although the toxicities are clearly linked with additional disease and financial burden [38], some studies did not report toxicity data and there were only 12 included studies explored the toxic effects of Act-D and MTX. Therefore, comprehensive characterization of toxicities would be needed for recognizing adverse events and enhancing life quality in the future clinical studies [39].
Some limitations of this meta-analysis should be stated. Firstly, heterogeneity between the included studies was generally present in this meta-analysis, manifesting in the difference of drug dosages and cycles, criteria for defining complete response, pretreatment beta-hCG level, FIGO score, and follow-up time. However, subgroup analyses stratified by these factors were not possible because of unavailable information. Retrospective design of some studies was the inherent bias, while the results of subgroup analysis for complete remission were consistent with the pooled result that obtained from all studies. Secondly, adverse events data were collected and graded according to different criteria, including CTCAE, WHO, and Gynecologic Oncology Group toxicity criteria. Few studies did not mention the methods for collecting adverse events, possibly depending on investigators' evaluation or self-reporting by patients. Additionally, some treatment-related adverse events were not fully reported, we therefore could not make analyses for the toxicities. Thirdly, most of the studies have been performed by Asian and Latin America institutions, limiting the interpretation of the results for western populations. Fourthly, the meta-analysis was based on summary data extracted from published articles and not on individual patient data. Finally, meta-analysis is inherently observational and it is possible that the results are affected by unmeasured cofounding factors.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}