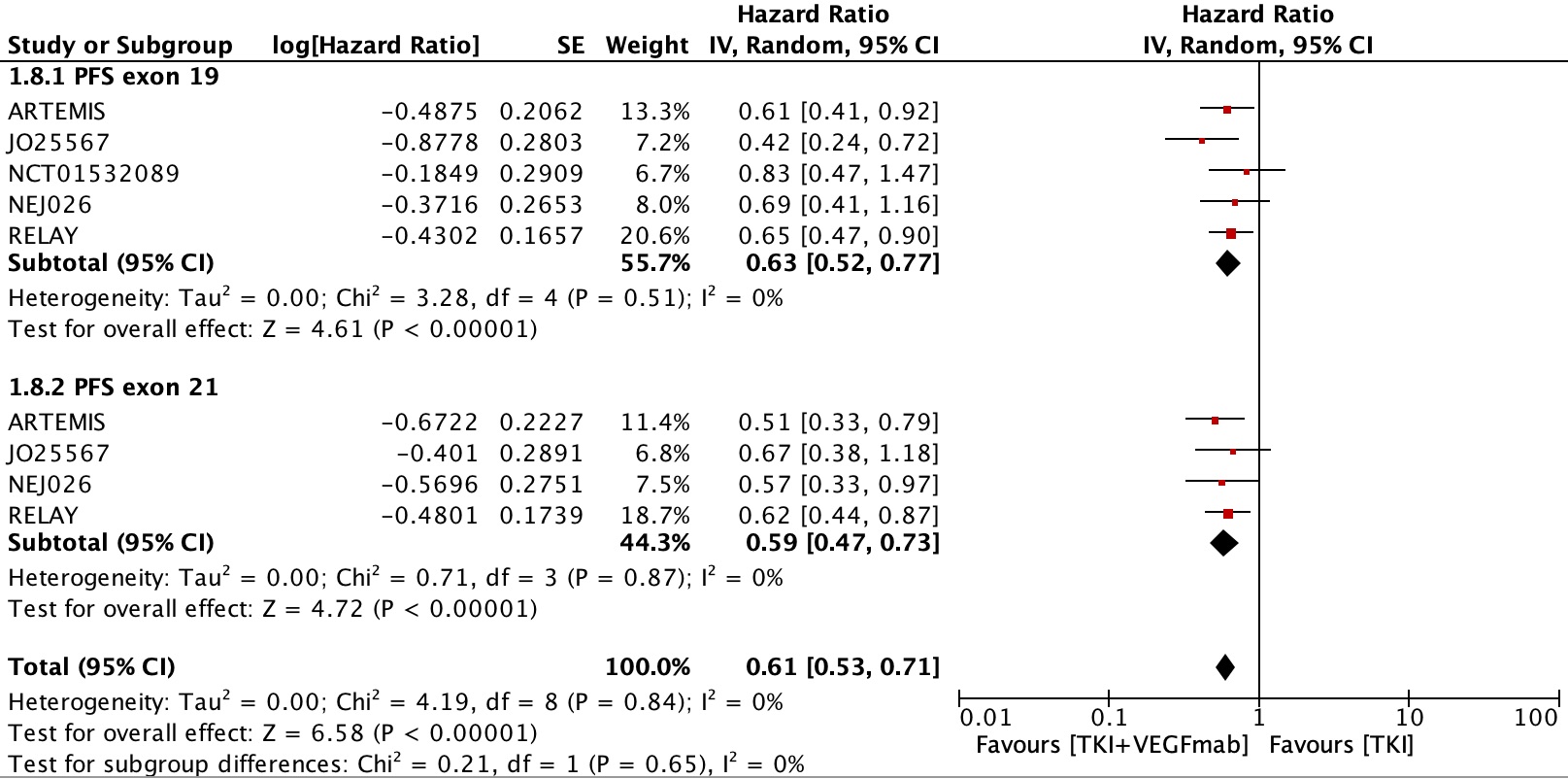
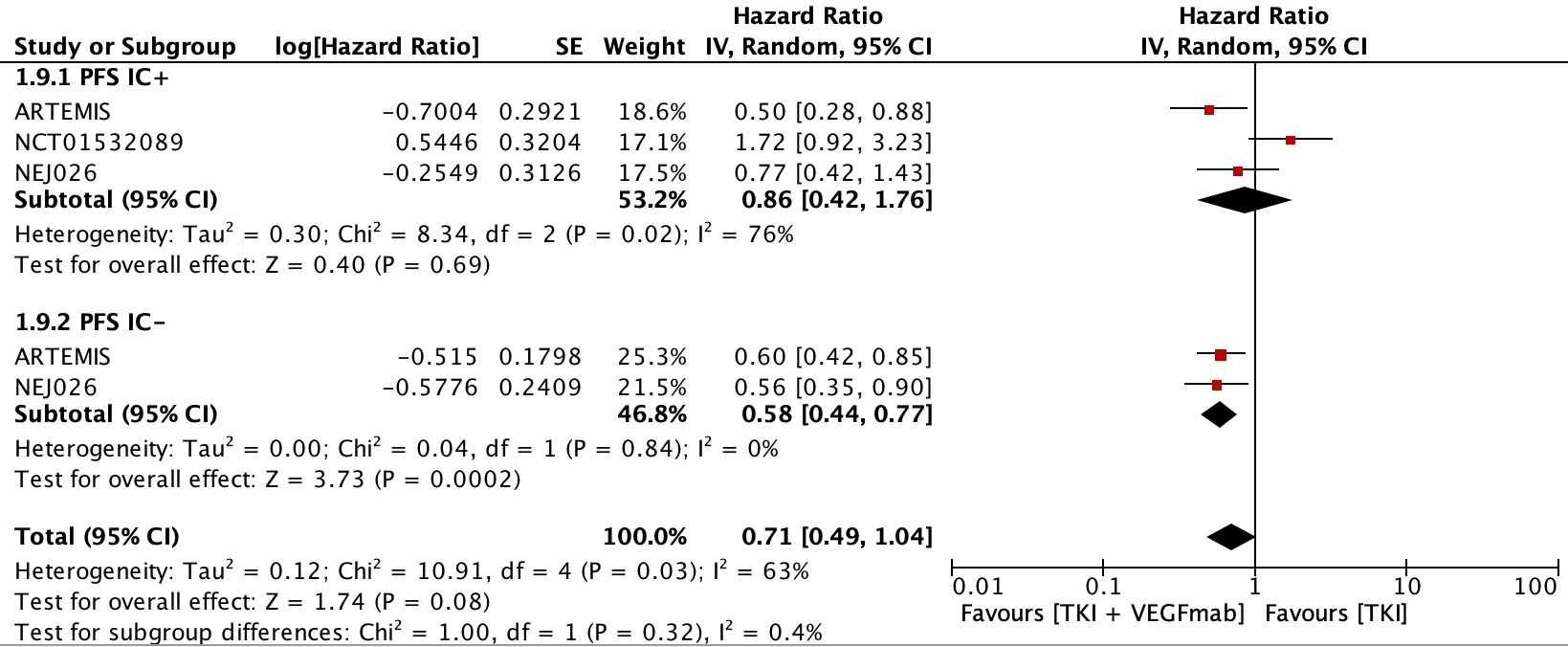
This meta-analysis was conducted to assess the efficacy in terms of PFS and OS for the combination of EGFR-TKIs and VEGF inhibitors in advanced NSCLC harboring activating EGFR mutations compared to the standard of care treatment with EGFR-TKIs alone. The results of this study demonstrated that combined inhibition of EGFR and VEGF pathways in patients with an EGFR activating mutation in advanced NSCLC significantly prolongs PFS, and was evident across all subgroups. Notably, the BAGEL trial[13] had opposing PFS results compared to the other trials analyzed. The population size for this trial was quite small, and no hazard ratio was reported in the paper which is why it was not included in the forest plot analysis. The reported PFS HR of 0.62 in this meta-analysis can be clinically meaningful; however, the clinical meaningfulness was defined by the American Society of Clinical Oncology[27] for patients with advanced NSCLC as an improvement of at least 4 months in PFS and a hazard ratio for OS of < 0.80 with minimal additional toxicity. In most trials, the 4 months improvement in PFS was met but the OS outcome is not clinically meaningful yet as it did not reach statistical significance.
No difference in OS was observed between the combination treatment and EGFR-TKI alone. Unfortunately, some trials had not reported OS data, or it was not yet mature. In the RELAY trial for example, mOS was not met in either group, but the hazard ratio for interim analysis was still reported and included in our analysis. The lack of mature OS data, as well as treatment with subsequent lines of therapy including patients in the control arms crossing over to receive anti-VEGF treatment, could in part explain why there was no significant difference in mOS between groups. If there truly is no difference in OS between groups, it would raise the question as to whether sequential treatment with single agents may be just as effective as combination treatment, but with reduced toxicity.
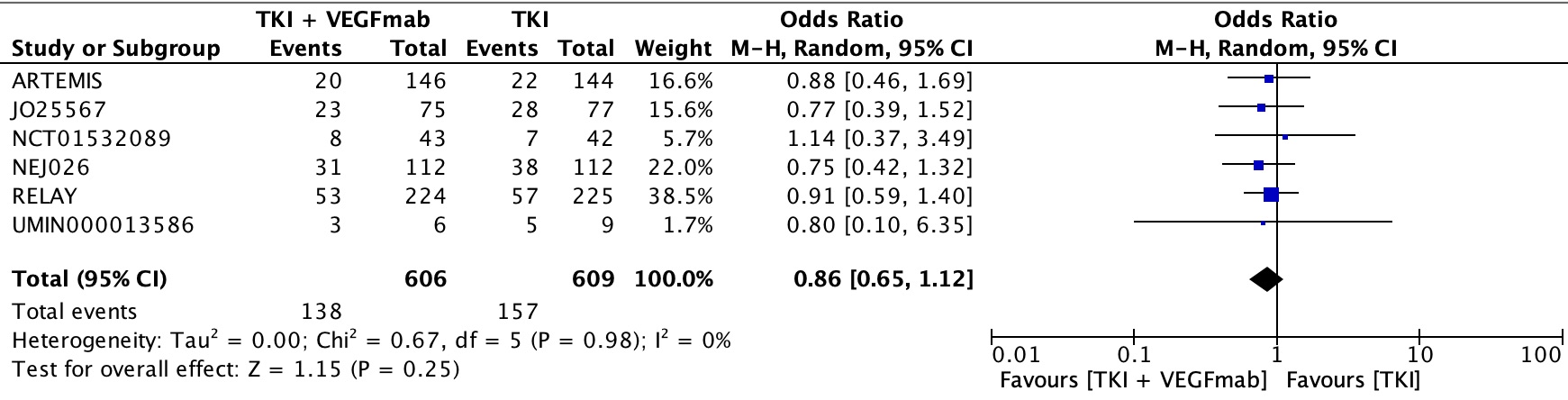
Disappointingly, there did not seem to be an improvement in ORR or DCR. One would have hoped that by targeting two separate mechanisms of tumor growth, the number of responders would increase, however, this was not observed. As these trials were examining patients in the first line setting prior to development of resistance, it is possible blockade of dual pathways which share the same downstream effects would not increase response rate. Acquired resistance has not yet developed in patients starting first-line treatment, so the addition of VEGF inhibitors would not have a role in overcoming resistance and increasing response rate for that reason. In the pre-clinical trials, the VEGF pathway is suppressed with EGFR blockade initially, until resistance develops, and the pathway attenuates[4].
Conversely, a large proportion of acquired resistance is due to T790M mutations. It’s possible that VEGF attenuation only accounts for a small portion of acquired resistance, with other mechanisms of resistance predominating. Osimertinib was initially utilized in the second line setting as its mechanism is not affected by T790M mutations, and thus could overcome acquired resistance from the development of such a mutation. It is now also approved for use in the first line setting as it was shown to have superior survival outcomes as compared to earlier generation TKIs and had a superior ORR and DCR compared to earlier TKIs[2]. While some of this improvement in response rates could be accounted for by patients with primary resistance due to de-novo T790M mutations, the proportion of patients with de novo mutations was small suggesting Osimertinib may be inherently better than other TKIs for reasons other than overcoming T790M. An early phase I/II open-label single arm trial examined Osimertinib and bevacizumab for treatment of EGFR mutant advanced NSCLC has found the combination to be safe and tolerable, with an ORR of about 80% and median PFS of 19 months, but the results were not compared to monotherapy Osimertinib in a randomized fashion and cross trial comparisons are difficult[28]. A more recent trial conducted examined the combination of Osimertinib and bevacizumab compared to Osimertinib alone in patients with T790M mutations who had progressed on earlier generation TKIs and found that the addition of bevacizumab did not improve progression-free survival in this setting[29]. Interestingly, response rates improved, but progression free survival was shorter in the combination treatment arm[29]. This could potentially be accounted for by prior exposure to TKIs leading to cross-resistance to anti-VEGF treatments, and the authors noted that they allowed for enrollment of participants that had previously received anti-VEGF treatments[29]. Results in first line setting comparing combination Osimertinib and anti-VEGF treatment to standard first-line Osimertinib are awaited.
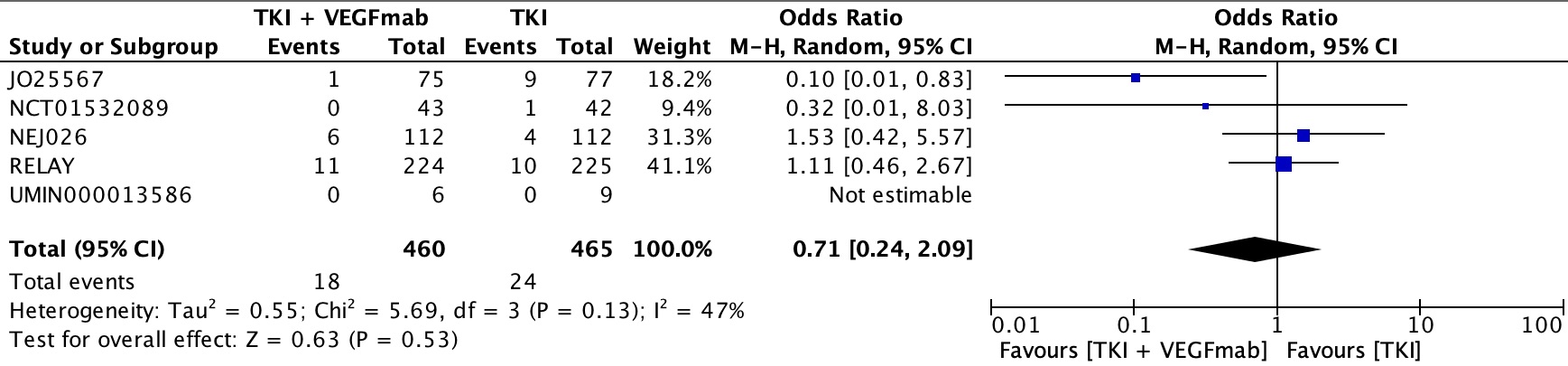
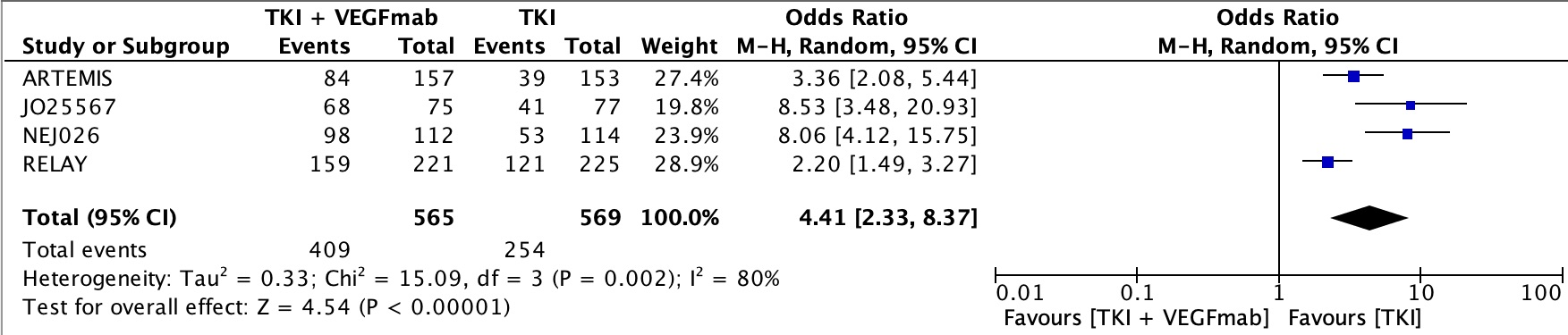
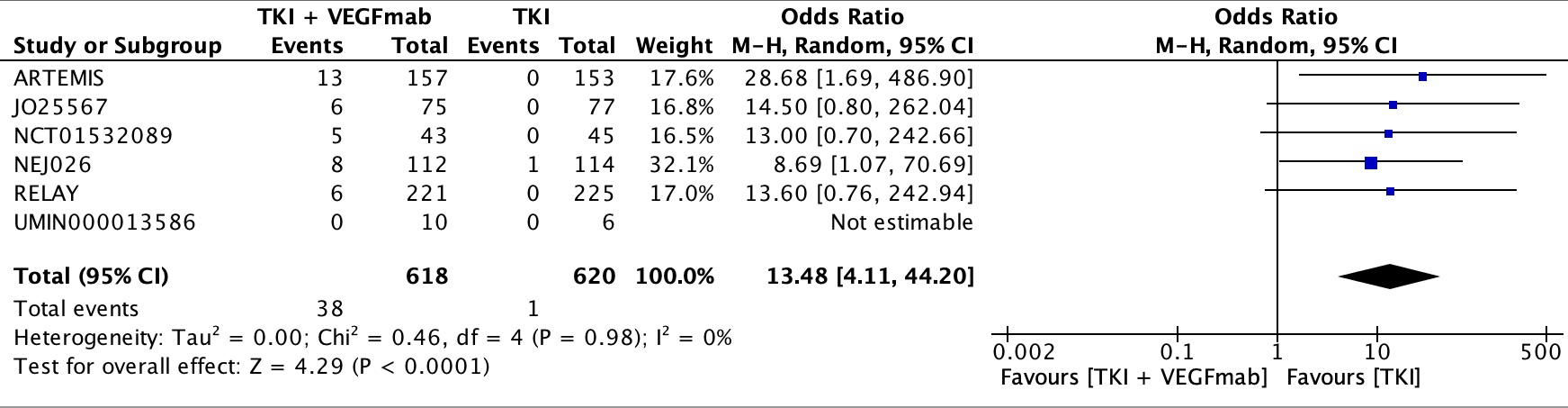
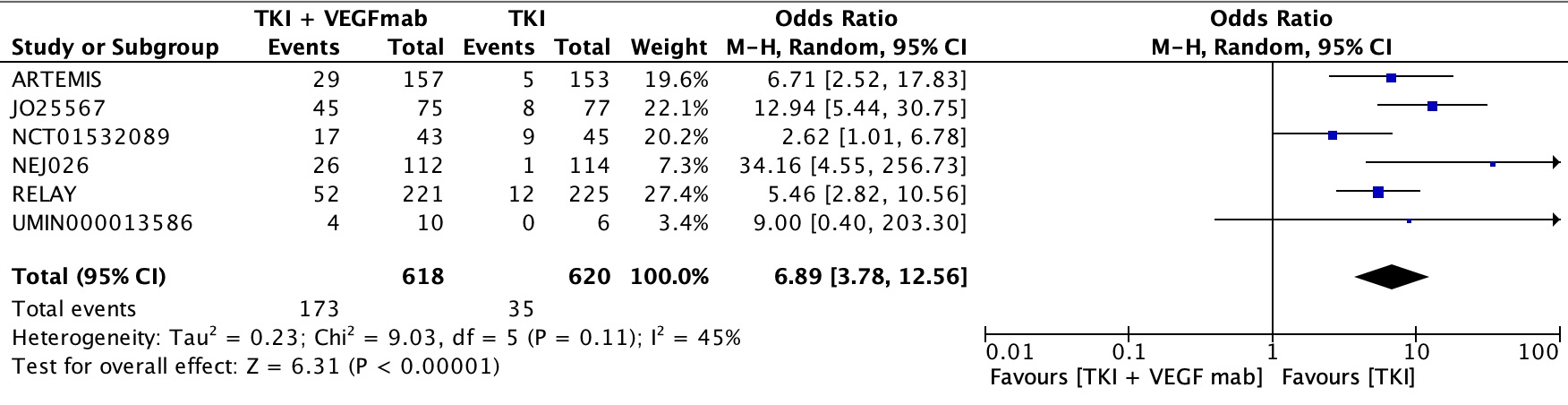
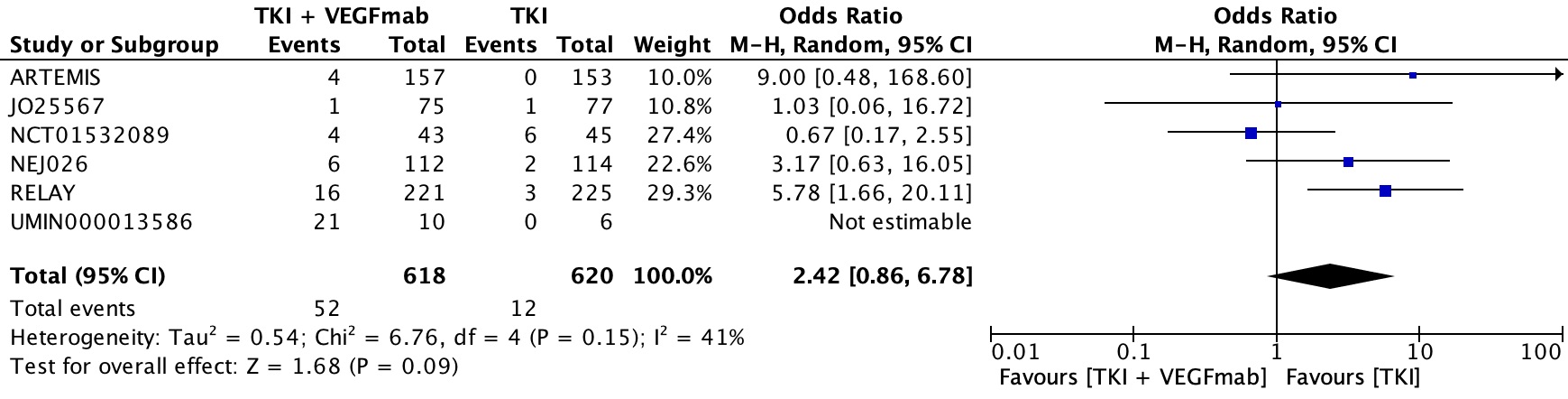
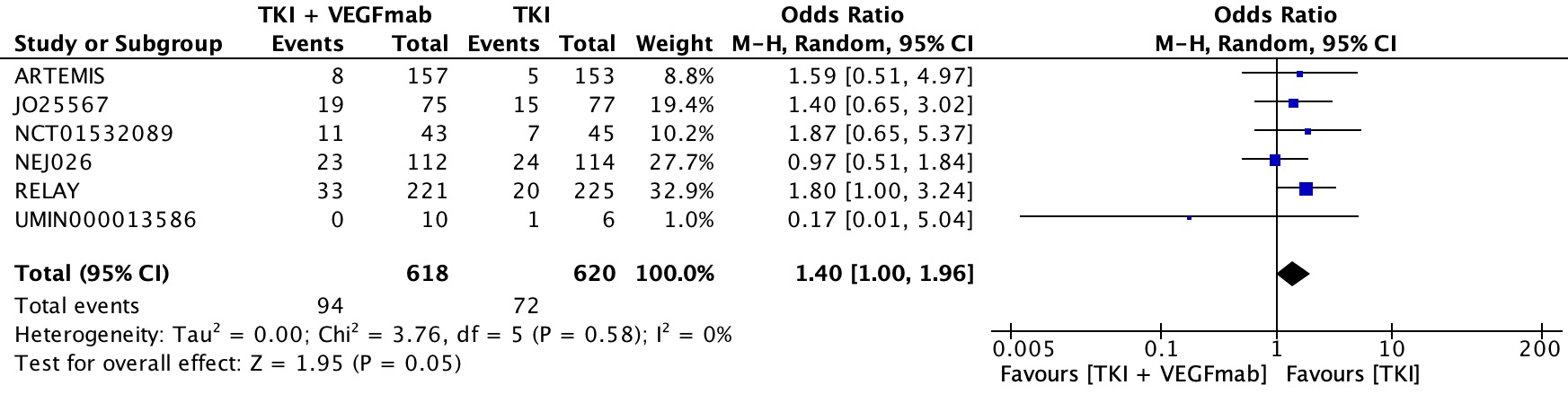
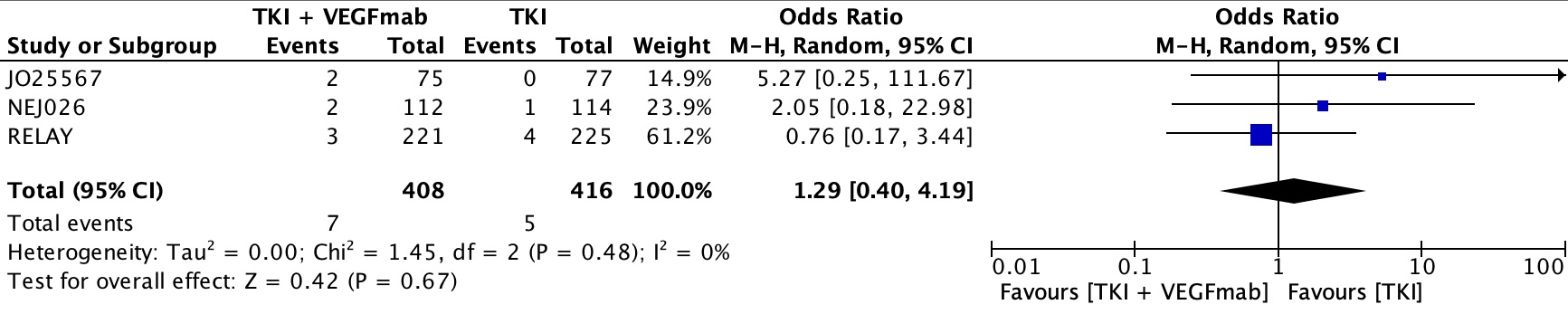
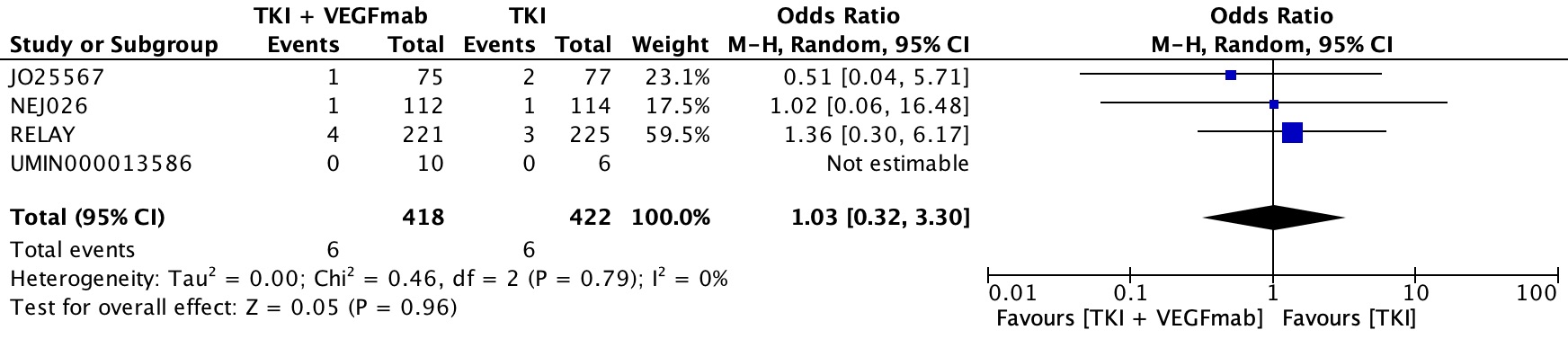
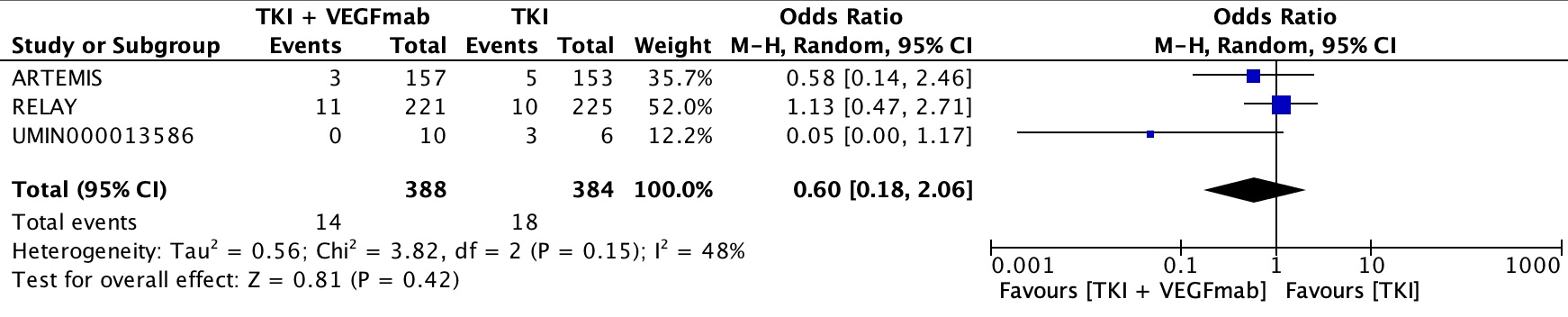
In our toxicity analyses, the combination treatment was reasonably well tolerated, although more toxic than EGFR TKI alone, with hypertension, diarrhea and proteinuria being the most frequent cause of grade 3–4 toxicity. Without including information on quality of life, it is unclear whether the improvement in PFS also translated to a meaningfully improved quality of life for patients, or whether the toxicity experienced outweighed the potential benefit of disease stability. One of the trials recently reported quality of life data, however, showing that time to treatment failure was similar between the experimental and control arms, and that the only patient reported symptom that differed was increased hemoptysis in the experimental arm, likely due to the addition of the antiangiogenic agent[30]. The potential benefit in PFS without an OS benefit, and increased toxicity, would also have to be weighed against the expense of adding a VEGF inhibitor when appropriate parties are deciding whether to fund this combined regimen.
A limitation to this analysis is that there were no trials comparing combination VEGF and EGFR inhibition with osimertinib as the control arm, which is the new standard of care based on the FLAURA trial[2]. Since this trial only was published in 2018, there were not any phase III trials with this combination either with osimertinib in the treatment combination arm or as a control arm comparator. There are currently early phase clinical trials and randomized trials underway examining this[28].
Another limitation is that there were some trials in this analysis which included patients with brain metastases and other trials which did not, which could result in heterogeneity in the overall survival analysis. Furthermore, the older generation TKIs do not have substantial blood brain barrier penetration compared to osimertinib, and in theory, including osimertinib in this combination could have improved results.
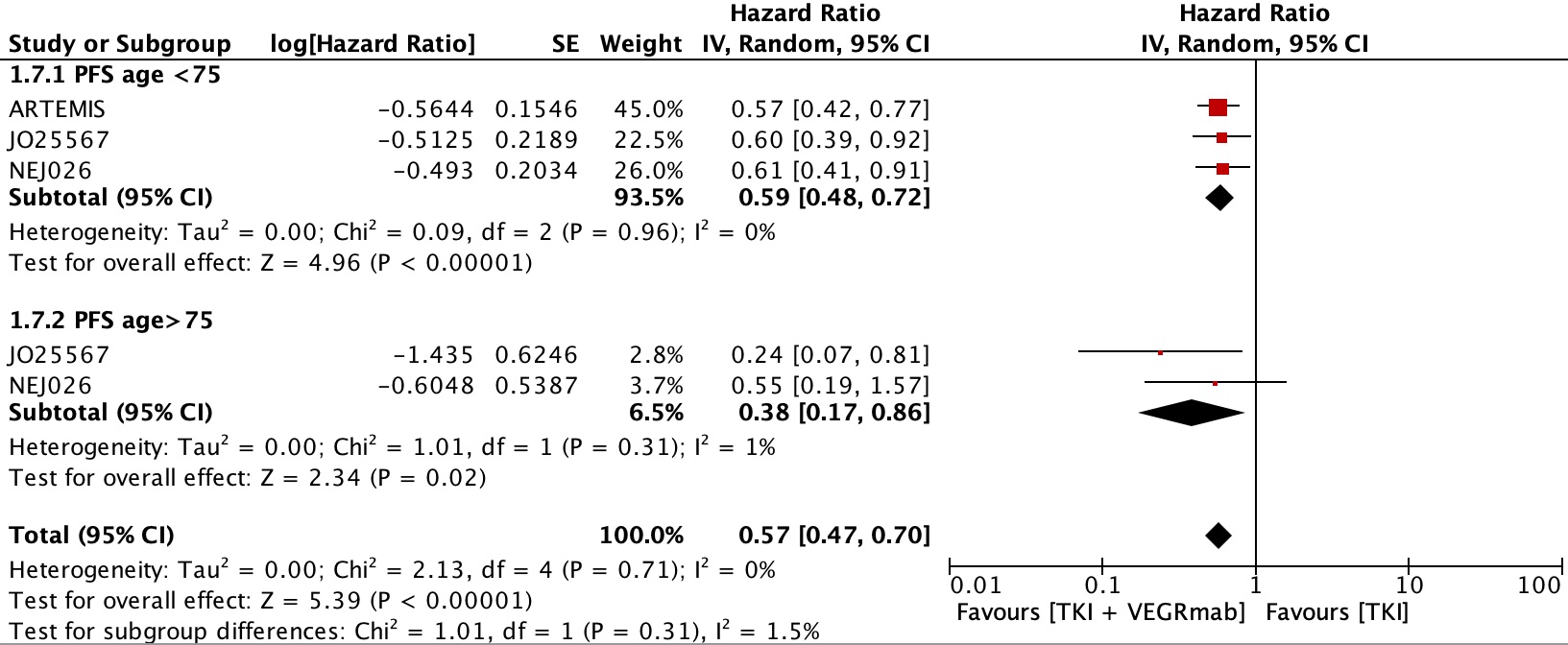
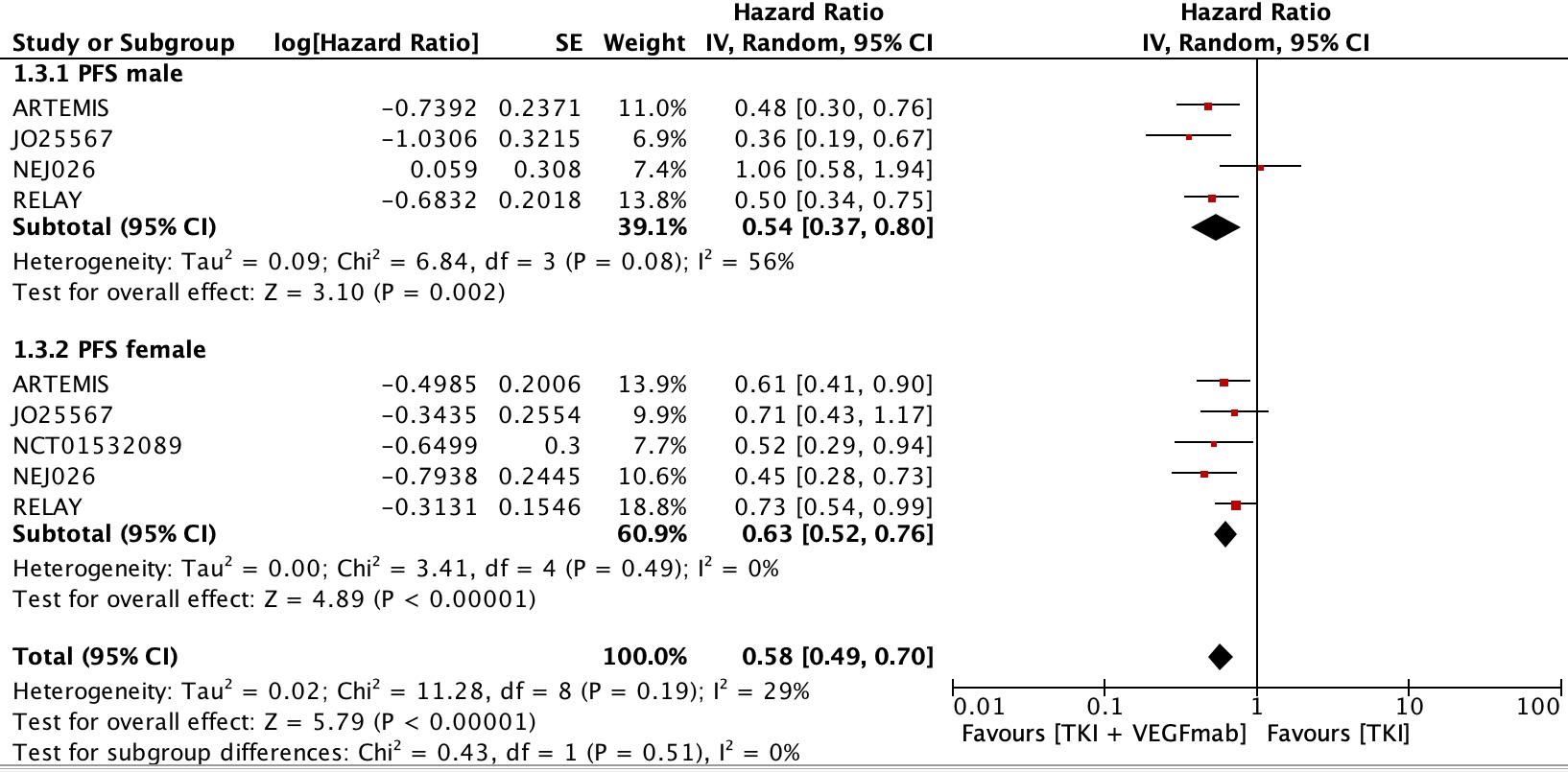
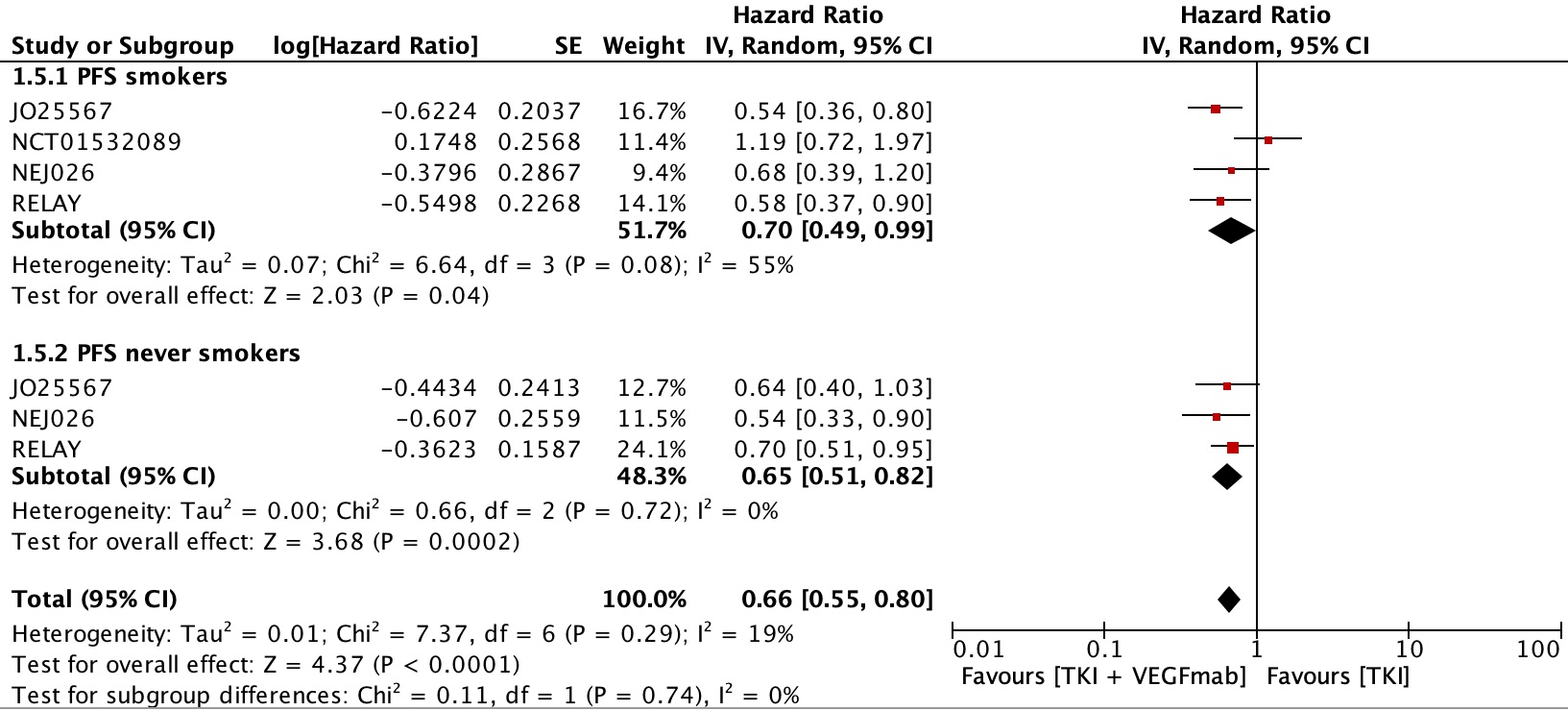
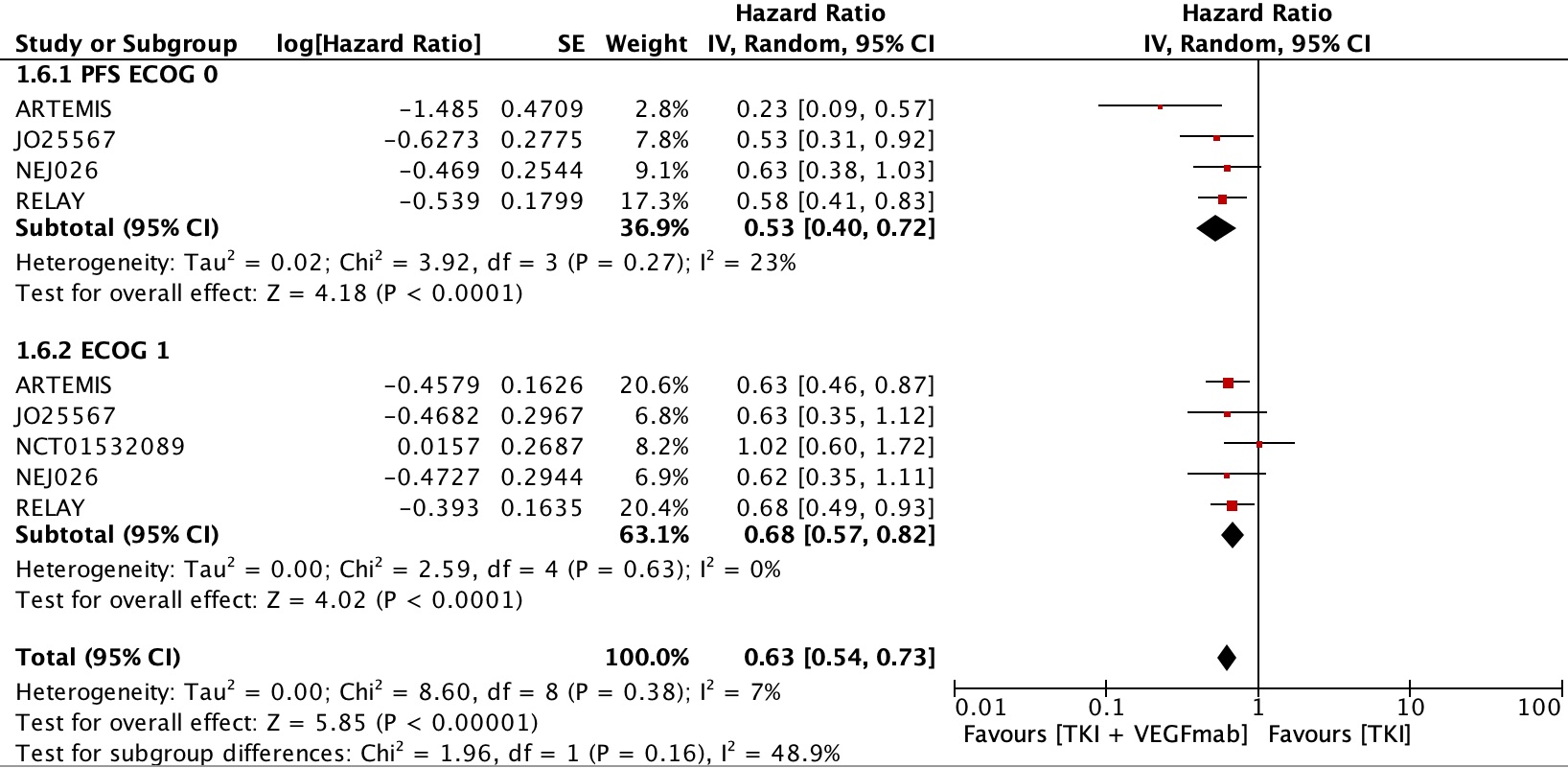
The subgroup analyses were of course limited by the small number of studies that were included. This was further compounded by varying definitions of variables which did not allow for direct comparison. For example, some studies defined smoking status as non-smokers or smokers, while others include never smoker and past smokers as variables. Moreover, the use of summary data rather than patient-level data weakens the possibility of discovering meaningful associations and reaching stronger conclusions.
A strength of our meta-analysis is that it adds to the literature compared with previous meta-analyses examining this combination in that we have limited our studies to only those with populations whose tumors were screened for EGFR activation mutations, since we know that EGFR TKIs have improved efficacy in those tumors, and we excluded studies whose control arm included VEGF inhibitors or chemotherapy, thereby improving the homogeneity of included trials. Prior meta-analyses included trials that had participants both with and without mutations. Since we know that EGFR TKIs have improved efficacy in those tumors with confirmed activating mutations, trials with mixed populations potentially diluted the efficacy of EGFR TKIs.
In summary, the level of recommendation to support offering a combination treatment with EGFR TKI and VEGF inhibitor is moderate. More research is needed to examine this combination with newer generation EGFR TKIs such as Osimertinib, which has prolonged PFS and improved central nervous system (CNS) penetration, and to also include osimertinib as the new standard of care for the control arm in the first line setting. Furthermore, improved efficacy in PFS alone may not warrant a change in clinical practice without an accompanying overall survival benefit, as sequential treatment could potentially have similar outcomes in survival but with less toxicity[31]. Quality of life data would also be important to consider if there is no change in overall survival benefit. the addition of mature OS data is needed to confirm and strengthen the results of these findings.
In conclusion, combined inhibition of first EGFR TKIs in combination with VEGF inhibitors results in a clinically meaningful benefit in PFS but not OS with mild toxicity. However, given osimertinib is the new standard of care in the first line setting, further research is warranted to assess whether combined inhibition of EGFR with osimertinib and a VEGF inhibitor results in improved survival outcomes in addition to mature OS data from the previously published trials.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}