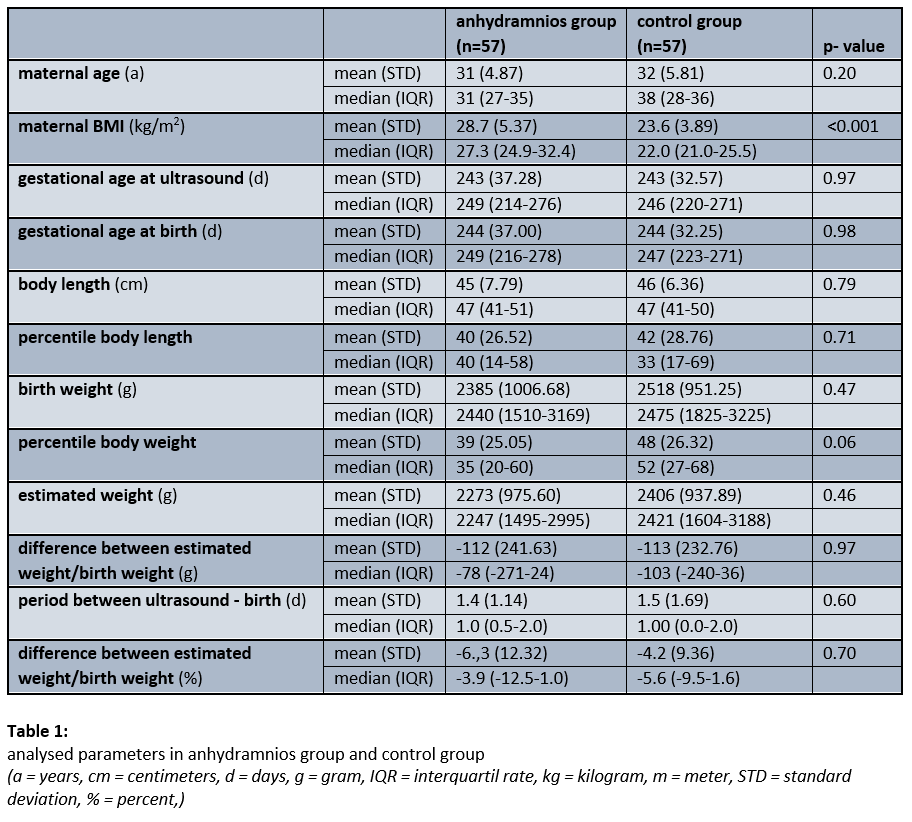
With this case-control study, we were able to demonstrate that the presence of anhydramnios does not significantly worsen the measurement accuracy of the estimated fetal weight, regardless of gestational age. Illustrated by Bland-Altman-plots, the mean difference as well as upper and lower limits of agreement between sonographically estimated and birth weight were almost identical.
We performed the sonographic weight estimation based on Hadlock's formulas, which showed a small deviation from the actual birth weight. We opted for a maximum of a five days interval (range 0–5 days) between sonographic weight estimation and birth, which is between the limits also used in comparable current publications [Ben-Haroush 2004, Faschingbauer 2015, Hoopmann 2016, Esin 2017, Janas 2019].
In 2015, Faschingbauer et al. conducted a study on 8721 singletons with the aim of determining the accuracy of common estimation formulas (Hadlock I, Hadlock II, Merz, Shepard, Warsof) and the influence of the time interval between weight estimation and birth. They were able to show that Hadlock's formulas, which tends to generally underestimate actual weight, predict birth weight most accurately if the scan was performed within a week before birth [Faschingbauer 2015].
In 2016, Hoopmann et al examined 35 common estimation formulas in a cohort of 3416 singleton pregnancies with an estimated fetal weight between 2500 and 4000g. They were able to confirm that formulas according to Hadlock (III and V) show the smallest percentage deviation on average. The maximum interval between the scan and birth was seven days [Hoopmann 2016].
It is well known that obesity has no influence on the measurement accuracy. Because of this we did not adjust the results for maternal BMI. The fact that the case group even had a higher BMI and that there was no difference between the EFW and the birth weight under this condition underpins the observations of current publications: Maternal obesity seems not to have an adverse effect on the measurement accuracy [Huber 2014].
Our results show for the first time that anhydramnios does not significantly affect the sonographic measurement accuracy of fetal biometry. In both patient cohorts, the sonographically determined fetal weight tended to be underestimated, i.e. the actual birth weight was slightly higher. The fact that a reduced amount of amniotic fluid has no significant effect on the accuracy of EFW is consistent with publications in recent years. However, only patients with oligohydramnios or a generally reduced amount of amniotic fluid were examined up to now.
In 2004, Ben-Haroush et al found in a study of 131 pregnant women with oligohydramnios at term that oligohydramnios had no effect on the accuracy of the EFW. Measurements taken no more than 3 days before birth were included. A uniform formula was not used [Ben-Haroush 2004].
In a study of 234 pregnant women, Esin et al. demonstrated that oligohydramnios did not affect the accuracy of estimated fetal weight measured within 7 days prior to delivery. Weight formulas according to Hadlock showed the lowest median estimation error [Esin 2017].
Janas et al. found in a study of 1831 pregnant women that the amount of amniotic fluid had no impact on the accuracy of estimating fetal weight. Women who had an ultrasound within 48 hours before birth were included. In oligohydramnios (n = 229), there was a non-significant tendency to overestimate fetal weight [Janas 2019].
In a study with 106 pregnant women, Duncan et al. were able to show that the measurement accuracy does not decrease significantly when the amount of amniotic fluid is reduced. In the subgroup analysis of patients with anhydramnios (n = 26), the percentage deviation of estimated weight from birth weight increased non-significantly [Duncan 2020].
By confirming that anhydramnios has no influence on the difference between estimated fetal weight and birth weight in an accurately performed fetometry, our results are particularly relevant for decision-making in the management of extremely preterm births. In the early weeks of pregnancy at the limit of viability between 22th and 24th weeks of gestation, the fetal weight plays an important role in assessing the prognosis. An estimation that is as accurate as possible helps the attending obstetricians and neonatologists to come to a joint decision with the parents-to-be regarding the optimal obstetric management and the postpartum neonatological care of the premature child.
A birth weight below 500g is particularly critical. Smith et al. conducted a prospective cohort study in 12 clinics in Belgium, France, Italy, Portugal and the UK on this topic in 2017. 1449 premature babies between 22 + 0 and 25 + 6 weeks of gestation who were born in 2011 and 2012 were included. The premature babies were divided into groups according to gestational age (in complete weeks of pregnancy) and birth weight over and under 500 g. It could be shown that regardless of the birth weight, no preterm infant born in 23th week of pregnancy survived despite intensive medical efforts. From the 24th week of pregnancy, the probability of survival in the weight class < 500g is less than 25%. None of the surviving children survived without serious impairments [Smith 2017].
A more detailed explanation of the role of birth weight was provided in a large Canadian retrospective cohort study from 2011. Data from 17 148 preterm infants (born between 22th and 32th weeks of gestation) who were treated in neonatal intensive care units in Canada between 2003 and 2008 were analysed. The primary endpoint was discharge without severe impairment (severe neurological impairment, chronic lung disease, retinopathy ≥ 3°, necrotizing enterocolitis ≥ 2°). It could be shown that female gender, higher gestational age at birth and higher birth weight are independent positive predictors of a good outcome. Based on the data, a graph was created for male and female preterm infants, showing the probability of surviving without serious impairment in relation to gestational age at birth and the birth weight. The probability to survive without a handicap when a baby is born at 25th week of gestation was less than 5% for male babies with a birth weight < 500g, < 10% with a birth weight of 600g and around 15% with a birth weight of 750g. Correspondingly, female preterm infants have a significantly better prognosis with a probability to survive without a handicap of 10% with a birth weight of 500 g, 15% with 600 g and 20% with 750 g [Shah 2011].
The presented studies point out that an accurate sonographic weight estimate is important for assessing the prognosis of extremely preterm born newborn. Our results illlustrate that even in the case of anhydramnios, EFW does not deviate from EFW of pregnancies with a normal amniotic fluid volume.
{kind=link}