Patient 1: A male patient who is 75 years-old with chronic renal disease and myasthenia gravis transferred from a long-term care facility with respiratory failure on 21 February 2019. On day eleven of admission, B. cepacia was isolated from a tracheal aspiration sample. The patient was diagnosed with ventilator-associated pneumonia (VAP) due to B. cepacia, and treatment with piperacillin-tazobactam was started and continued for ten days. The patient improved, but the patient deceased on admission day 55.
Patient 2: A 85 years-old male patient with Alzheimer's was admitted with community-acquired pneumonia to another healthcare facility. Later he was transferred to the ICU. Respiratory samples grew B. cepacia on day 21 of admission. The patient did not fulfill the VAP criteria. On admission day 80, the patient developed VAP due to Acinetobacter baumannii and died on day 95.
Patient 3: A 86 years-old female patient with sigmoid adenocarcinoma underwent re-laparotomy due to an anastomose leak. The patient was diagnosed with intraabdominal sepsis and treated with piperacillin-tazobactam and vancomycin. On admission day two, B. cepacia was detected in the tracheal aspirate. Antimicrobial treatment for intraabdominal sepsis was streamlined to piperacillin-tazobactam and levofloxacin. The patient recovered from intraabdominal infection and was discharged to the surgical ward on admission day 23 and eventually discharged from the hospital on day 25.
Patient 4: A male patient who is 69 years-old with diabetes was admitted with subacute anterior myocardial infarction to the intensive care unit. He underwent left anterior descendent artery stent placement. The patient was intubated due to respiratory insufficiency. On admission day eight, B. cepacia was isolated from respiratory cultures, and the patient was diagnosed with VAP. Cefepime was started then de-escalated to levofloxacin. He received 14 days of antimicrobial treatment. The patient died on admission day 45.
Patient 5: A male patient who is 73 years-old with chronic obstructive pulmonary disease and chronic renal failure was admitted to the ICU on 24 January 2019. The patient was diagnosed with community-acquired pneumonia and treated with ceftriaxone and clindamycin. B. cepacia was isolated from tracheal aspirate on admission day 60. Levofloxacin treatment was started and continued for ten days. The patient was deceased on admission day 130.
Patient 6: A male patient who is 77 years-old, operated on 21 January 2019 for cervical spinal stenosis. The patient was admitted to ICU with septic shock on 05 February 2019. On day 56 of admission to ICU, B. cepacia was isolated from deep tracheal aspirate culture. The patient died on the same day. Retrospective examination showed death was not related to a HAI due to B. cepacia.
The six patients' timeline between admission, detection of B. cepacia, and discharge/death is displayed in Figure-1.
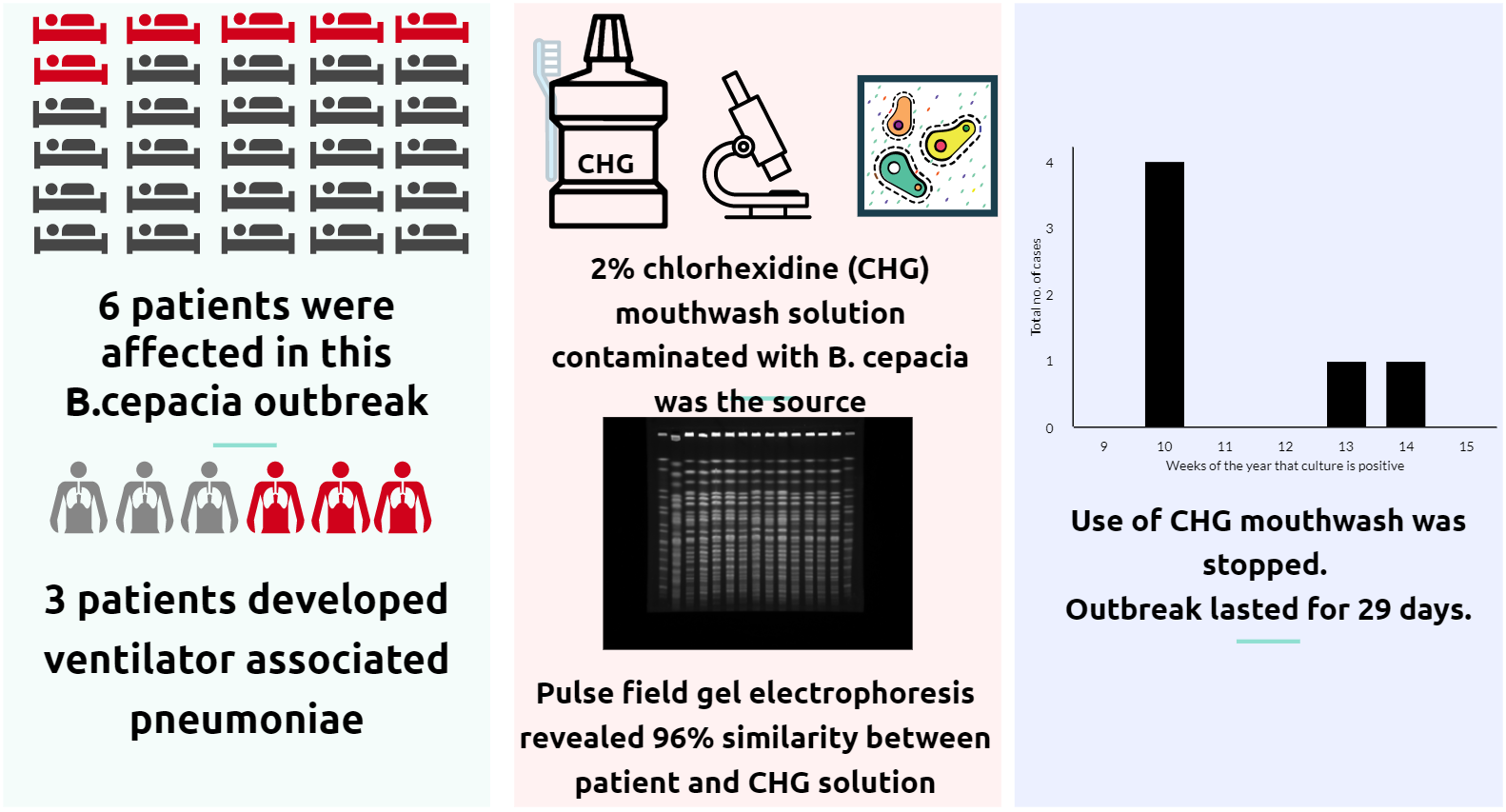
In total, we took 34 environmental samples and six hand cultures from HCW. B. cepacia was detected in opened mouthwash products in affected and unaffected patients in the unit. Additional samples were taken from unopened products in the ICU and central storage units. B. cepacia was detected in unopened products. Contamination was detected in all samples (17/17) of a specific batch (G05) of the mouthwash solution. In total, 17/20 of opened and unopened products showed growth. Three unopened solutions without growth had a different batch number (G11). The G05 batch was in use on 24 February 2019 (during the preceding two weeks). The remaining 14 environmental cultures showed no growth other than Pseudomonas aeruginosa and Serratia marcenses from sinks. Cultures from hands of the HCW showed no significant growth.
Overall, six patients became colonized, and three of them developed VAP. The median age of colonized patients was 76 (25–75%: 73.5–86). The median time to colonization from admission to ICU was 17.5 days (25–75%: 7.7.5-48.25).
Figure 2 shows the PFGE dendrograms of B. cepacia isolates from the patients and the mouthwash solutions. The PFGE detected five pulsotypes out of 20 B. cepacia isolates. There was a 90% similarity between the two clusters. The isolates in the second cluster had a %96 similarity.
Interventions and measures taken:
We contacted the neighboring hospitals using the same product. They reported no additional B. cepacia cases. We recommended to cohort all colonized patients in the same section of the unit. The use of the product was stopped throughout the institution. IPC monitored the hand hygiene compliance of the unit and gave feedback to HCWs during the outbreak. Infection prevention strategies to prevent HAIs was reminded to the staff. The outbreak lasted 29 days, and no further clusters were identified after discontinuing the contaminated solution.
{kind=link}