There are differences in CRC screening strategies due to differences in geographic variation of CRC prevalence, available funds, and health infrastructure [23, 24]. The impact and economic evaluations are great from early detection of CRC [25, 26]. However, many countries still lack effective CRC prevention and screening programs at the national level. Thus, the CRC screening program was implemented nation-wide in SA.
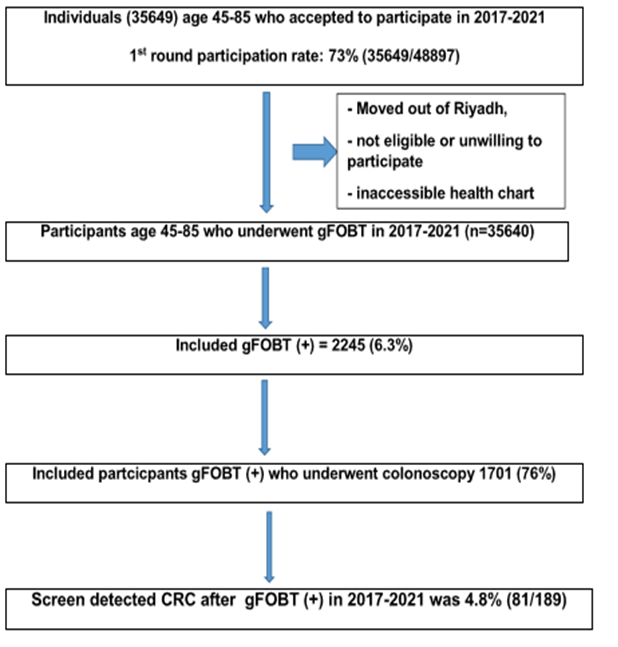
The CRCSP intends to help prevent CRC in central area of SA, Riyadh and its surrounding region Al-Kharj province of Riyadh—Riyadh the most populated area in SA. CRC screening programs using pure endoscopy and pathology are not appealing to a wide range of people because the method is invasive. This in turn leads to a lack of involvement. In our study, 20% of the subjects refused to undergo colonoscopy despite a positive HSgFOBT results. One recent study [28] reported that about 33% of scheduled colonoscopies were postponed during a period of 16 months because of encompassing personal, social, geographic, and health system factors. Here, the performance of colonoscopy was within two weeks: There was no delayed colonoscopy after the initial positive HSgFOBT becuase this delay was associated with poor outcomes due to CRC [29]. Second-round CRC screening will continue according to recommendations [16, 22].
In a local study, 71% of Saudis preferred CRC screening using the following modalities in descending order: CT colonography (CTC), stool based-test, colonoscopy, and flexible sigmoidoscopy [31]. Similar to our study results, there was a preference for HSgFOBT and then scope-based methods [31]. Furthermore, based on their investigation of CRC awareness among healthy individuals in SA, Zubaidi et al. strongly recommended implementing a countrywide policy including an education/screening program to improve CRC knowledge [4]. Reasons included misconceptions regarding universally-accepted screening protocols, atypical symptoms, and awareness of CRC disease in SA in general.
There is a lack of national data in the literature from SA on the frequency of adenomatous polyps and the age groups most affected. The prevalence of CRC in our study was 4.8%, advanced adenoma was 9.5%, adenoma was 15.9%, non-adenoma polyps was 7.9%, and no polyps or tumors was 25.4%.
Another retrospective cohort study reported adenomas at 8.1% and advanced adenomas at 0.5% [26]. Most adenomas (33.9%) were located on the left side of the colon. Similar results have been reported in a retrospective study reporting that 25% of the patients diagnosed with rectal tumors and the majority 42.89% with left colon [32].
In this screening study, the Saudi population has a mean age of 50.5 ± 15.9 yo with a female predominance of 57.7%. Higher frequencies relative to our study were expected because our study involved a general population being screened for CRC.
A recent retrospective study from 2009 to 2017 reported a significant increase in the incidence of late onset CRC between 2009 and 2011 (28.46%) and 2012–2014 (35.47%); folloed by a drop from 2015 to 2017 to be 32.51% [32].
In other studies there is a decrease of late onset cancer at ages more than 50 years old [33]. In our study the total ASR was 3.2/100,000, for males 4.1/100,000 vesrus females 2.3/100,000. Compare with an older study at 2004 [33], the highest ASR were much higher Riyadh region 9.6/100,000. Other areas with high ASR were in Eastern regioon 9.8/100,000, Northern region 9.6/100,000, Makkah region at 7.4/100,000 and Tabuk region 8.2/100,000.. The median age at diagnosis was 60 years among males with age between 19–105 and 58 years among females with age between 16–100 years. The ASR has decreased in ages more than 50 years old but early onset cancer is still much lower than in developed countries in contrary to our recent updated findings after 2017..
A meta-analysis of six observational studies reported that there is low-quality evidence of colonoscopy referring to 34 serious complications per 100,000 CRC screening procedures. In particular, 2.8 serious complications per 1,000 were reported for colonoscopy including perforation, bleeding, and even death. The authors concluded that invasive CRC screening modalities should only be undertaken at specilazed centers with skillful and experienced clinical staff for advanced therapeutic endoscopy. However, no complications were reported in our study.
The first round of non-invasive assessment using the g-FOBT highlighted the strength and weakness of current clinical practices: the low number of referrals for CRC, the use of a non-invasive CRC screening test, and the unwillingness of HSgFOBT (+) individuals to proceed to structural tests; there was a low participation in SA relative to the international guidelines [22]. The high number of referral of patients at risk for CRC for endoscopy provided by local endoscopy services in the Al Kharj area combined with the second structural screening for CRC will decrease the incidence of CRC in Al Kharj by detecting premalignant and early stage cancers sufficiently before they grow to advanced. The outcome of CRC strongly depends on the stage at which it is detected; thus, those at risk for CRC must be motivated to undergo endoscopy.
The weakness of this study is that it was conducted to adopt the CRCSP in a large area of Riyadh province Al-Kharj, the capital of SA, but this approach is not yet a part of a national policy study for CRC screening. The sample size is small, but there is no limitation in applying the program in more hospitals in Riyadh for larger numbers of participants over a longer period after public education. Other limitations to be considered is the survivor cancer care and availability of molecular characterization of tumors and testing necessary to improve the outcomes of young patients with CRC. The assessment of patient-level information such as education, income, obesity, physical activity, was not performed because our analysis was based on aggregate data but still useful for assessing cancer rate trend.
One of the strengths of our data that there is no prospective study to assess the trends in CRC incidence frequencies among the young Saudi < 50 yo representing the 85% of the population. Our study showed low rates in CRC from 2017–2021 versus earlier years; there is no data available after 2016. The decrease in incidence frequencies could be possible attributed to the utility CRC cases in registries of other studies vs. the policy of population-based CRC screening since the initial CRC guidelines published in 2015. There is a high incidence in early onset CRC as reported in other studies with female predominance. One study was from northern area of Saudi Arabia although the study is retrospective and the sample represented all available colorectal cancers during a period of ten years.[7] and one also retrospective from Saudi National Registry before 2016 [6]. Our study reflects the global concern of early-onset CRC [16] with poor outcomes [34].
In conclusion, we detected a low incedence of CRC and advanced adenomas in the first round of CRC screening, thus highlighting a fall in CRC incidence in late onset CRC but an increase in early onset cancer. Participation in CRC screening was low. Subsequently, public education program is highly recommened along with endsocpy resources.
{kind=link}