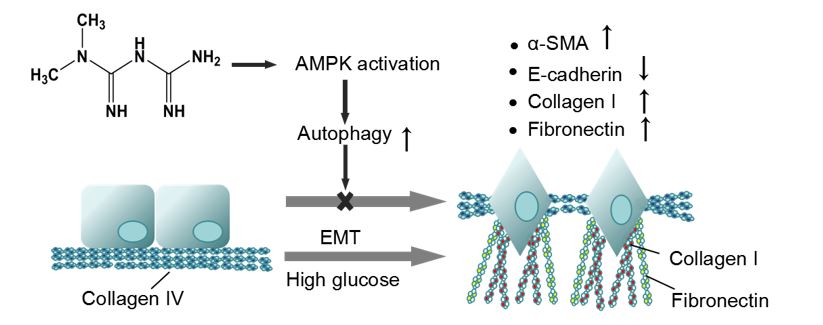
The therapeutic effects of metformin on slowing the progression of DN have been another spotlight apart from its hypoglycemic effects [28–30]. An initial objective of the study was to investigate the effect of metformin on TIF because it is still controversial [31]. The results indicated that metformin could significantly attenuate TIF and improve the level of autophagy in vivo especially in the early stage of DN, and inhibit the EMT of high-glucose-treated RTECs in vitro. Furthermore, our results explained the relationship between the autophagy and EMT, and confirmed that metformin could activate the AMPK especially in the early stage of DN, leading to the improvement of renal autophagy and reduction of EMT, thus significantly slow the progression of DN.
Previous studies showed metformin could inhibit fibrosis in several organ systems [32–36]. Gamad et al [37] found metformin could suppress pulmonary fibrosis via activation of AMPK by metformin. Li et al [38] reported that metformin attenuated the fibrogenic response of hepatic stellate cells in vivo and in vitro by activating AMPK. Cavaglieri et al [39] demonstrated metformin prevented renal interstitial fibrosis in rats with unilateral ureteral obstruction by the way of activating AMPK. Besides, Herzig et al [40] reported that autophagy machinery involves several multi-protein complexes that control every step, and AMPK regulated various aspects of this machinery. The findings described above were in line with our results and we provided further evidence to confirm the anti-fibrotic effects of metformin in the DN.
Although the results of this study showed that the level of fibrosis decreased with the increase of autophagy, but the changes in the corresponding pathways were not further explored. In a model of prolonged serum starvation of fibroblasts, Bernard et al [41] showed that sustained autophagy activates mTORC2 signaling, leading to enhanced expression and secretion of CTGF and the transformation of fibroblasts to myofibroblasts to favor the development of fibrosis. Furthermore, in TGFB1-treated primary human atrial myofibroblasts, autophagy was required for the induction of fibrotic signaling and the synthesis of both Collagen 2 and FN [42]. The results gave us inspiration that the catabolic machinery of autophagy is possible to participate in an anabolic process of protein synthesis, which had become the target of our further research.
Despite it had existed studies explored the pharmacodynamics of metformin on various fibrosis, there were a few researches on the therapeutic effects of metformin on different stages of DN. Our results showed that the functional biochemical parameters between 4-week DN group and 12-week DN group were of great differences. Specifically, we initially measured the body weight and KW/BW of DN model mice at 4 weeks and 12 weeks to roughly reflect the effects of metformin on different DN stages of the rats. The results showed the weight loss of mice in the early stage of DN was slighter, and the value of KW/BW was lower. This phenomenon indicated that the pathological changes of rats became more terrible as the course of DN prolonged. In order to further explore the changes in kidney function of rats at different stages of DN, we measured several classic indicators (24h-urinary protein, BUN, SCr). By reflecting the changes of biochemical indicators of renal function, we found that the decrease of renal function was consistent with the aggravation of DN, namely, with the development of DN, renal function continued to downgrade and the difference was obvious. Then, we studied the changes in the kidneys of DN rats to explore the causes of changes in renal function. According to the results of H&E, the morphological changes in the end stage of DN were more severe than those in the early stage, including more serious glomerular hypertrophy, mesangial matrix hyperplasia, renal tubule dilatation and inflammatory cell infiltration. At the same time, it was accompanied by more expression of renal interstitial fibrosis, including vacuolar degeneration, interstitial widening, interstitial fibrosis and excessive ECM deposition. In addition, the immunohistochemical and immunoblot results of College I and FN further confirmed that the level of renal fibrosis in the end stage of DN was significantly more aggravative than that in the early stage of DN. Interestingly, although there were still some differences from normal conditions, the pathological changes had been improved at varied degrees after metformin treatment, especially in the early stage of DN. It was reflected in the improvement of body weight and KW/BWT, the recovery of renal function, the weakening of renal morphological changes and the reduction of renal interstitial fibrosis. In order to investigate the potential mechanism of metformin, we explored the effects of metformin on autophagy and EMT in different DN stages. The results implied that metformin activated AMPK during the entire process of DN, increased autophagy flux and the number of autophagosomes, thereby enhance the level of autophagy in DN. Furthermore, in the RTECs stimulated by high glucose, metformin also showed the effect of activating the AMPK process to reduce EMT. The increase of autophagy and the accompanying reduction of EMT were more obvious in the early stage DN, while the effects were relatively weak in end stage of DN.
A possible explanation for these phenomena may be the function of metformin performing in the TIF. Metformin might play a role of preventing healthy cells or tissues from further lesions, rather than reverse the diseased parts back to the initial situation. Our results showed the pathological changes were relatively mild in the early stage of DN. In this case, metformin could protect mostly healthy cells or tissues from further deterioration so that the therapeutic effects on 4-week DN were more significant. However, if the progression of DN developed into the end stage, the therapeutic effects were limited because metformin could not reverse the formed lesions although the use of metformin was still effective.
In summary, the present study demonstrated that metformin had protective effects on STZ-induced diabetic rats. These beneficial effects were mediated through the activation of autophagy and suppression of EMT. The therapy of TIF was successfully achieved by the activation of autophagy offered by metformin in the early stage of diabetic TIF. The results provided new ideas for the treatment of diabetic renal tubulointerstitial fibrosis.
{kind=link}