Since NAC chemotherapy is currently an accepted treatment for breast cancer, including early-stage breast cancer, markers with prognostic and predictive value on the basis of NAC have been resarched [25, 37]. The importance of the Ki67 expression level as a prognostic factor in breast cancer has been demonstrated in many studies [20, 38].
pCR is an end point of NAC and is used as an independent prognostic marker [39].
However, there are also differences between studies [39–41]. The strongest correlation between pCR and survival was reported in aggressive tumours [39, 40]. The results are inconsistent in the luminal subtypes, while pCR is correlated with prolonged survival, especially in the triple-negative and HER2-positive subtypes [13, 41]. Von Minckwitz et al. [4] reported that pCR was significantly correlated with prolonged DFS in luminal B HER2-negative, HER2-positive and triple-negative tumours, but no such correlation was found in luminal B HER2-positive and luminal A tumours. One of the reasons for the differences among studies may be the use of different criteria for pCR. In some studies, only the response of the breast is taken into account, while in others, the lymph node response is also taken into account along with the breast response. There should be no residual tumour in breast and in lymph node for pCR in the RCB classification. In contrast, the lymph node is not considered in evaluation in the MP grading system [9, 34]. Hence, it is crucial to optimize the whole process as a multidisciplinary approach. However, the histopathological evaluation method is not usually stated in the literature [41, 42]. Luminal A tumours, which have low pCR rates, have a good prognosis and low chemosensitivity [43]. It has been shown that a pCR is not prognostic in ER-positive tumours [44, 45].
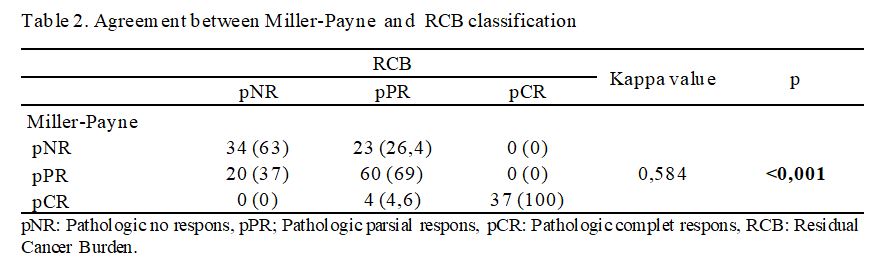
While the MP grading system evaluates treatment response according to the reduction in cancer cellularity, the RCB classification evaluates tumour response based on the tumour diameter, tumour cellularity, and axillary lymph node status [9, 34]. For this reason, the compatibility of the two evaluation systems was investigated [46, 47]. Romero et al. [46] found a high correlation between the MP grading system and the RCB classification in their study, where they compared the two treatment response assessment systems. They also found a correlation between the MP and RCB systems and survival [46]. We found a moderate correlation between the MP and RCB response assessment systems in this study. There is some difference between the response groups since there are differences in the evaluation criteria of the two systems. In this study, no correlation was found between the degrees of treatment response and survival in either system. Similarly, no correlation was found between MP grade and RCB score and survival in a study comparing treatment response systems [48]. Choi et al. [49] compared 7 different treatment response assessment systems and found all systems to be correlated with OS and DFS in their study. When evaluated in molecular subtypes, they found that only the RCB system was correlated with OS and DFS in all subtypes. This finding suggests that evaluation of breast and lymph nodes together is better correlated with the clinical course [47, 49]. All systems were significantly correlated with OS and DFS in the triple-negative group. We found no correlations between treatment response and OS and DFS in either system.
Data regarding the importance of the Ki67 index in predicting pCR are controversial [25, 26]. It has been reported that tumours with a high pretreatment Ki67 index have a higher pCR rate [27, 28]. Balmativola et al. [25] found that the pretreatment Ki67 index was higher in the pCR + pPR group than in the pNR group in their study, in which they grouped treatment response as pNR and pCR + pPR. They found that the cut-off for the Ki67 index, which distinguishes pNR patients from pPR and pCR patients, was 18% [25]. It was reported that patients with a Ki67 index of less than 25% were nonresponders to treatment and that DFS was longer in tumours with a Ki67 index of less than 12% in a study showing that the Ki67 index is correlated with pCR [30]. Acs et al. [27] reported that the Ki67 index and subtype were significantly correlated with pathological response, and NAC was more effective in tumours with a Ki67 index of at least 20%. In their study, the cut-off value for Ki67 was found to be 15% when OS was taken into account, but no Ki67 cut-off correlated with DFS was found [27]. The pCR rates were 4.2%, 12.8%, and 29% in a study grouping the Ki67 index as low (≤15%), moderate (15.1–35%) and high (>35%), respectively [37]. Evaluation of all the patients in this study revealed that in the hormone receptor-positive group, OS and DFS were longer in tumours with a low Ki67 index. However, it has been reported that such a correlation was not observed in triple-negative tumours [37].
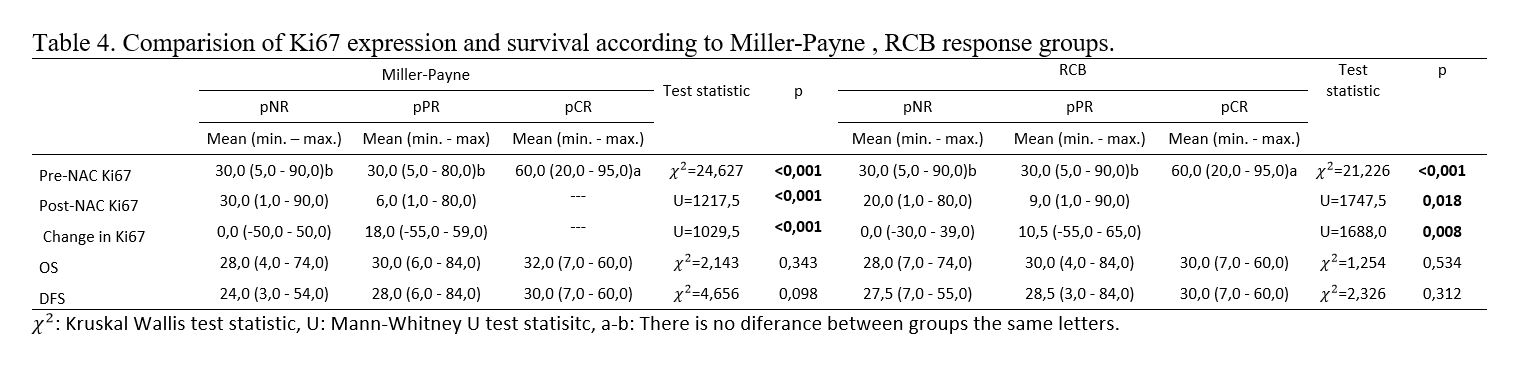
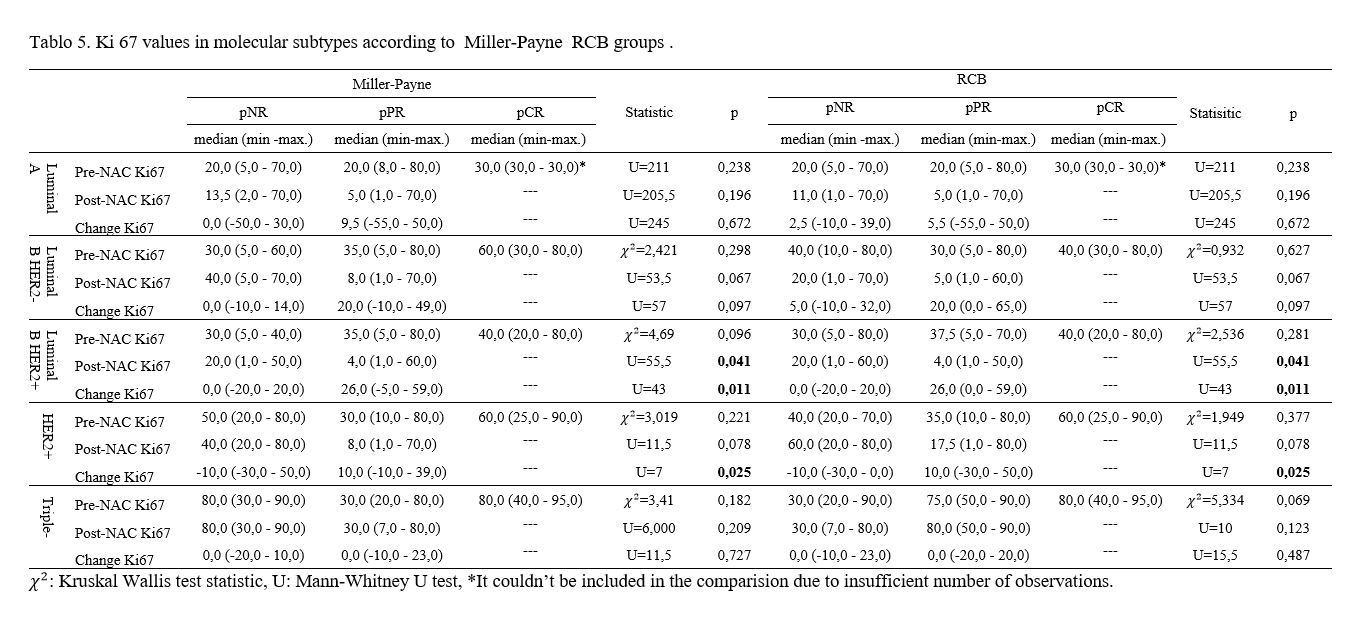
Zhao et al. [50] reported that a high Ki67 index was a strong predictor of pCR in their study of HER2-positive tumours. The Ki67 index was correlated with the degree of pathological response in this study. In our study, the pretreatment Ki67 value was found to be higher in the pCR group than in the pPR and pNR groups in both the MP and RCB classification systems. We identified a Ki67 cut-off for pCR of 37%. We could not find a Ki67 value that distinguished pNR patients from pPR and pCR patients.
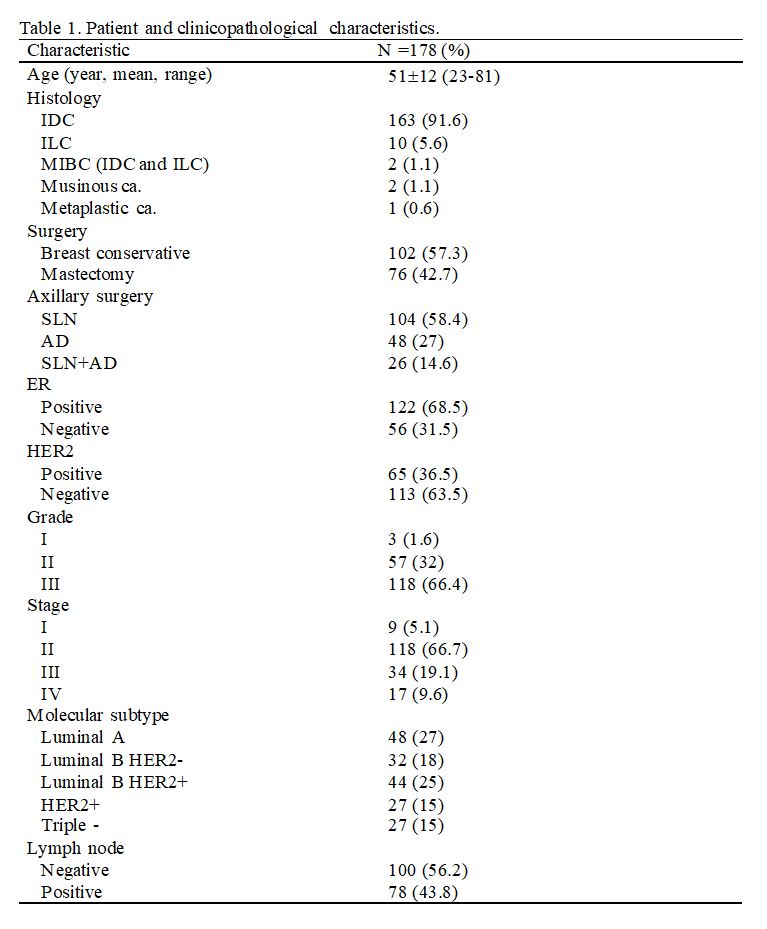
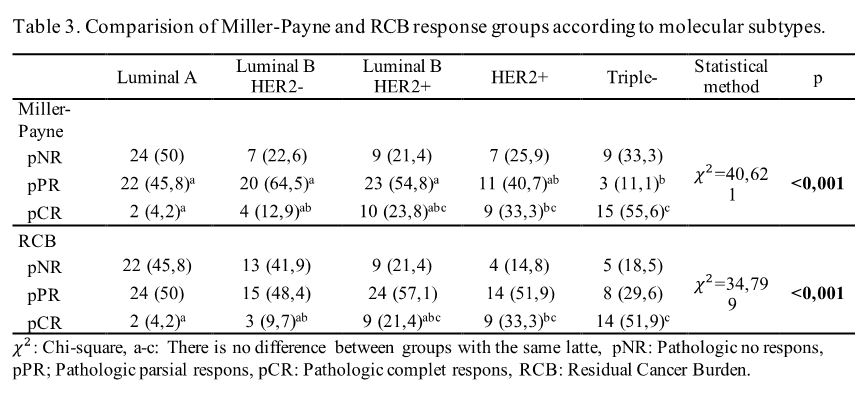
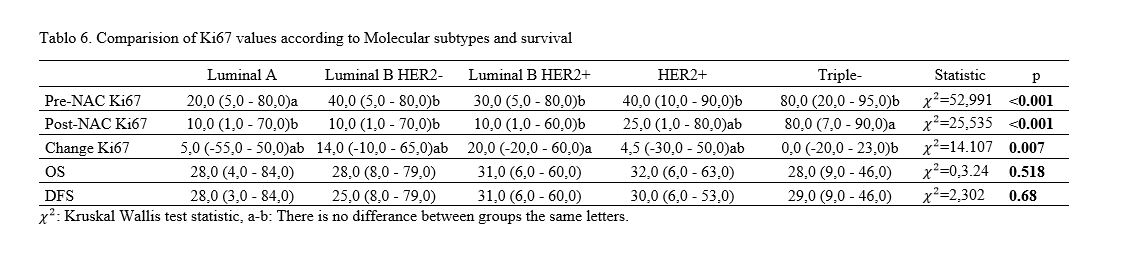
The treatment responses of the molecular subtypes were correlated with those in the literature [25]. In our study, triple-negative tumours had the highest pCR rates. HER2-positive tumours ranked number two. The lowest pCR rate was in luminal A tumours, while the luminal B HER2-negative subtype was ranked number 2. Luminal A tumours, which had the lowest pCR rate in our study, had the lowest pretreatment Ki67 index values. The triple-negative molecular subtype, which had the highest pCR rate, was the group with the highest pretreatment Ki67 index values. No correlation was found between MP and RCB grades and pretreatment Ki67 values in the molecular subtypes in our study. Luminal B HER2-negative tumours are tumours of intermediate category, and endocrine therapy is recommended for all these patients and cytotoxic therapy for the majority of these patients [19]. Multigene analyses are performed on adjuvant and neoadjuvant grounds to distinguish patients who are likely to benefit from chemotherapy [51, 52]. The evaluation of the cell cycle-specific antigen Ki67 by immunohistochemical methods in the evaluation of the proliferative activity of tumours has been widely studied. It has been shown that patients with luminal B/HER2-negative tumours with a high proliferation index benefit from chemotherapy [21, 37, 53]. In our study, we could not find a correlation between the pretreatment Ki67 proliferation index and treatment response in the luminal B HER2-negative subtype. However, we found a negative correlation between pretreatment Ki67 and disease-free survival in the luminal B HER2-negative subtype. Zong et al. [54] also reported that the DFS of luminal B HER2-negative tumours with a high Ki67 index was shorter than that of the group with a low Ki67 index. They also reported that they did not observe a correlation between OS and the Ki67 index, similar to our study [54]. Ki67 should be considered for the selection of more aggressive treatment modalities in luminal B HER2-negative tumours [54].
The evaluation of residual disease after NAC is important not only to identify patients who should receive additional adjuvant therapy but also to identify the subgroup with a good prognosis among patients with this residual disease [7, 13]. It has been reported that posttreatment Ki67 expression levels are associated with prognosis [3, 7, 13, 32, 55]. Especially in tumours where the prognostic value of pCR is limited, a prognostic predictor such as Ki67 in residual tumours has gained importance. It has been reported that patients with low Ki67 levels in residual tumours after NAC have a similar prognosis to patients with pCR(5). Nishimura et al. [30] reported in their study that there was a significant decrease in the Ki67 value after neoadjuvant treatment and that patients evaluated as clinical complete response had a lower Ki67 value after treatment. Assersohn et al. [56] reported that the level of Ki67 at excision is correlated with prognosis in tumours that do not respond completely. In our study, when we evaluated the Ki67 value without division by molecular subtypes, the posttreatment Ki67 index was found to be higher in the pNR group than in the pPR group. When we evaluated the molecular subtypes separately, the posttreatment Ki67 index of the pNR group was found to be higher than that of the pPR group in the luminal B HER2-positive molecular subtype. Von Minckwitz et al. [5] reported that high posttreatment Ki67 levels were correlated with relapse and death. They reported that the posttreatment Ki67 level was more prognostic than the pretreatment Ki67 level and the change in the Ki67 level after NAC in their study. They found that posttreatment and pretreatment Ki67 levels were correlated with residual tumour size [5]. In our study, a negative correlation was found between the posttreatment Ki67 index and OS only in the HER2-positive subtype. Similarly, in our study, the residual tumour size was correlated with the posttreatment Ki67 level. However, unlike that in their study, there was a negative correlation between the residual tumour size and the pretreatment Ki67 level in our study. This result is different from theirs and is compatible with the correlation between the pretreatment Ki67 level and the response we found in our study. Interestingly, a weak positive correlation was found between the posttreatment Ki67 index and OS in the luminal A subtype in our study.
It has been reported that DFS and OS are longer in patients with changed Ki67 expression than in patients with unchanged Ki67 expression [7, 57]. It has also been reported that the proliferative activity of tumours that respond to treatment is higher and that the proliferative activity decreases after treatment [58]. That study reported that the DFS was longer in tumours whose proliferative activity decreased by more than 30% after NAC [58]. It was reported that the change in the Ki67 level was prognostic in the luminal B, triple-negative and HER2-positive subtypes in the study of Matsubura et al. [57]. In accordance with the literature, while there was no change in the posttreatment Ki67 index in the pNR group, the Ki67 index was decreased in the pPR group in our study. However, no correlations were found between the Ki67 change and OS and DFS. In this study, the greatest decrease in the Ki67 index was observed in the luminal B HER2-positive subtype. A decrease was observed in the pPR group, while no change was observed in the pNR group in the luminal B HER2-positive subtype. While the posttreatment Ki67 increased in the pNR group of the HER2-positive subtype, it decreased in the pPR group. The Ki67 index showed no change in triple-negative tumours, in which we observed the highest response rate, in the pNR and pPR groups in our study. Diaz-Botero et al. [7] also reported that no decrease in the Ki67 index was observed in the pPR group in the triple-negative and HER2-positive subtypes with high pCR response rates [7]. Triple-negative breast cancer is an aggressive subtype of breast cancer with higher recurrence and metastasis rates than other subtypes [59]. In this group with an aggressive course, NAC allows to evaluate the chemotherapy response of the tumour before surgery. Triple-negative tumours, for which pCR has been achieved after NAC, have been reported to have a better prognosis than those without pCR [2]. In our study, while we found a correlation between the posttreatment Ki67 index and OS for only the HER2-positive subtype, we did not find a correlation in the triple-negative subtype. Although our study could not show its relationship with survival, different treatment options should be considered for triple-negative tumours that do not show a posttreatment Ki67 level decrease.
This study has some limitations. Although the number of our patients was not small, the decreased number of patients when divided into five molecular subtypes limited the evaluations between of molecular subtypes. In addition, our follow-up periods may have been insufficient for prognostic evaluation due to late recurrence of luminal tumours.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}