Response rate
In 2017, we identified 30 active adult EP labs in Canadian centres where cardiac ablations are performed; that number increased from 25 in the first survey installment. The response rate was 76% in original survey sent in 2012, 50% in the second installment in 2014, and 47% in 2016. Eleven centres have been consistently reporting their data in all 3 surveys, and are used in this analysis when comparing same data categories.
The identified EP centres are located in 9 of 13 provinces and territories; Prince Edward Island and three territories are served by external EP labs, typically located in neighboring provinces.
Laboratory Infrastructure and human resources
Table 1 provides a comparison of the infrastructure and resources trends 2011 to 2016 from all contributing centres.
Table 1
Facility Resource Information.
| |
2015–2016
|
2013–2014
|
2011–2012
|
| |
N (%)
|
N (%)
|
N (%)
|
|
University Affiliated Hospitals
|
14 (100%)
|
14 (100%)
|
17 (89%)
|
|
Lab Infrastructure
|
|
|
|
|
Centers: Implants done in OR
|
4 (29%)
|
6 (43%)
|
8 (47%)
|
|
Ablation rooms
|
1.9 (1–4)*
|
1.8 (1–3)*
|
1.6 (1–3)*
|
|
Days/Week Room used for Ablationa
|
7.0 (2–14)*
|
7.1 (2–14)*
|
5.3 (1–13)*
|
|
Implant Days/Weeka
|
3.4 (0–5)*
|
3.2 (0–5)*
|
3.25 (1–6)*
|
|
EP Procedures Performed
|
|
|
|
|
Diagnostic EP Procedures
|
14 (100%)
|
14 (100%)
|
19 (100%)
|
|
RF
|
14 (100%)
|
13 (93%)
|
19 (100%)
|
|
Contact Force
|
14 (100%)
|
n/a
|
n/a
|
|
Cryoablation point-by-point
|
12 (86%)
|
9 (64%)
|
n/a
|
|
Cryoballoon
|
10 (71%)
|
6 (43%)
|
15 (83%)
|
|
PVAC
|
3 (21%)
|
4 (29%)
|
n/a
|
|
NMARQ (circular RF)
|
2 (14%)
|
0
|
n/a
|
|
Mapping Systems
|
|
|
|
|
CARTO
|
12 (86%)
|
13 (93%)
|
14 (78%)
|
|
Intracardiac echo
|
12 (86%)
|
12 (86%)
|
14 (78%)
|
|
EnSite-NavX Velocity
|
10 (71%)
|
13 (93%)
|
15 (83%)
|
|
EnSite-NavX Precision
|
8 (57%)
|
n/a
|
n/a
|
|
Mediguide
|
2 (14%)
|
2 (14%)
|
n/a
|
|
Rhythmia™
|
1 (7%)
|
0
|
n/a
|
|
LocaLisa
|
1 (7%)
|
1 (7%)
|
1 (6%)
|
|
STXS
|
2 (14%)
|
1 (7%)
|
2 (11%)
|
|
Imaging Systems**
|
|
|
|
|
General Electric
|
1 (7%)
|
1 (7%)
|
n/a
|
|
Philips
|
8 (57%)
|
8 (57%)
|
n/a
|
|
Siemens
|
6 (43%)
|
7 (50%)
|
n/a
|
|
Toshiba
|
2 (14%)
|
2 (14%)
|
n/a
|
|
Portable GE
|
1 (7%)
|
1 (7%)
|
n/a
|
| * = range |
| ** = present in number of centres |
| a = days per week room used for ablation x number of rooms |
Data in the latest survey (n = 14) was from all university affiliated hospitals that perform EP studies and catheter ablations. Six centres (43%) perform EP procedures on pediatric (< 18 years) population. There was a slight increase in the average amount of EP enabled rooms since 2011 (mean 1.9 up from 1.6). On average, the equipped rooms are used specifically for ablation activity at 75% capacity in 2015–2016, while in 2011–2012 they were available for ablations only at 70% capacity (room was at 100% if used for ablation 5 days/week). Four of the 14 (29%) centres use the operating room for cardiac rhythm management device implantation, for an average of 3 days per week.
Ablation procedure types and mapping systems
Diagnostic EP studies and radiofrequency ablations were consistently performed in all participating centres since 2011; ablations using Contact Force catheters have been performed in all centres since 2015. Radiofrequency ablation remains the predominant technique; while the popularity of point-by-point cryoablation and balloon ablation have grown in the last 6 years. Please refer to Table 1 for usage rates of all modalities.
The survey collected data on imaging and electroanatomical mapping systems. CARTO and intracardiac echo were the most widely utilized in 86% centres, increasing from 78% of centres in 2011, followed by EnSite NavX-Velocity and EnSite NavX Precision utilized in 71% and 57% of centres respectively. Only one centre reported the current use of Rhythmia™ and one centre has continued to use LocaLisa since 2011. Two centres in Canada clinically use Robotic Magnetic Navigation systems (Niobe Stereotaxis, St. Louis, MO).
Personnel
In total, there were 57 full-time physicians (mean: 4.1, range: 0–7) who performed ablations in 2015–2016. Forty three percent of the responded programs employ 22 part-time physicians, with an average of 1.6 part timers per centre (range 0–12). The number of full-time and part-time EP staff have been increasing (from a mean of 3.5 to 4.1 full-time operators; 1.1 to 1.6 part-time operators per centre in the last 6 years).
There was a trend in more part-time electrophysiologists from 24–28% of total EPs. Ten of the fourteen (71%) hospitals employ 35 EP fellows, with an average of 2.5 trainees per centre. The ratio of teaching staff (full-time and pro-rated part-time) to trainees is approximately 2:1. We observed a trend of a decreased ratio between staff members and trainees over the polled time.
In 12 of 14 centres, there is an average of 4.6 nurses trained for EP procedures (range: 0–10); and an average of 3 permanent EP (range: 0–7). Seven (50%) centres employ EP technicians, with an average of 1.5 technicians per centre (range: 0–6). By 2016 non-3D mapping/recording systems became operated predominantly by EP nurses and industry reps, they are the primary operators in 50% and 29% of the centres respectively, EP techs operated 21% of the systems in 2016. Table 2 presents complete data on EP labs personnel.
Table 2
EP Laboratories Personnel data.
| |
2015–2016
|
2013–2014
|
2011–2012
|
| |
Mean
|
Range
|
Mean
|
Range
|
Mean
|
Range
|
|
Full Time physicians per centre
|
4.1
|
(0–7)
|
4.1
|
(1–7)
|
3.5
|
(0–7)
|
|
Part Time physicians per centre
|
1.6
|
(0–12)
|
1.2
|
(0–5)
|
1.1
|
(0–7)
|
|
Trainees per centre
|
2.5
|
(0–6)
|
2.9
|
(0–7)
|
2.7
|
(0–5)
|
|
Nurses trained specifically for EP
|
4.6
|
(0–10)
|
4.4
|
(0–10)
|
n/a
|
|
|
Permanent EP RN's
|
3.0
|
(0–7)
|
2.5
|
(0–6)
|
n/a
|
|
|
EP technicians
|
1.5
|
(0–6)
|
1.4
|
(0–7)
|
n/a
|
|
|
Non- 3D mapping systems operated by: N(%)*
|
|
EP technicians
|
3 (21%)
|
|
2.5 (18%)
|
|
9 (50%)
|
|
|
EP nurses
|
7 (50%)
|
|
7 (50%)
|
|
7 (39%)
|
|
|
Industry Reps
|
4 (29%)
|
|
4.5 (32%)
|
|
2 (11%)
|
|
| * = sums of totals, and percentage of total |
Procedural Data
Total procedures
In total, 7106 standard and complex catheter ablation procedures were reported annually for 2015–2016 by all responding centres, an average of 508 ± 270 per centre; this has significantly increased from 2011–2012, when the national average obtained by our survey was 421 ± 202 ablations. This is consistent with the increased number of rooms that are solely equipped for ablations, which have increased (mean = 1.9; (1–4) versus mean = 1.6; (1–3)), dedicated to ablations 7 days versus 5 days per week. Centres are steering away from doing implants in the operating rooms towards ablation labs (Table 1).
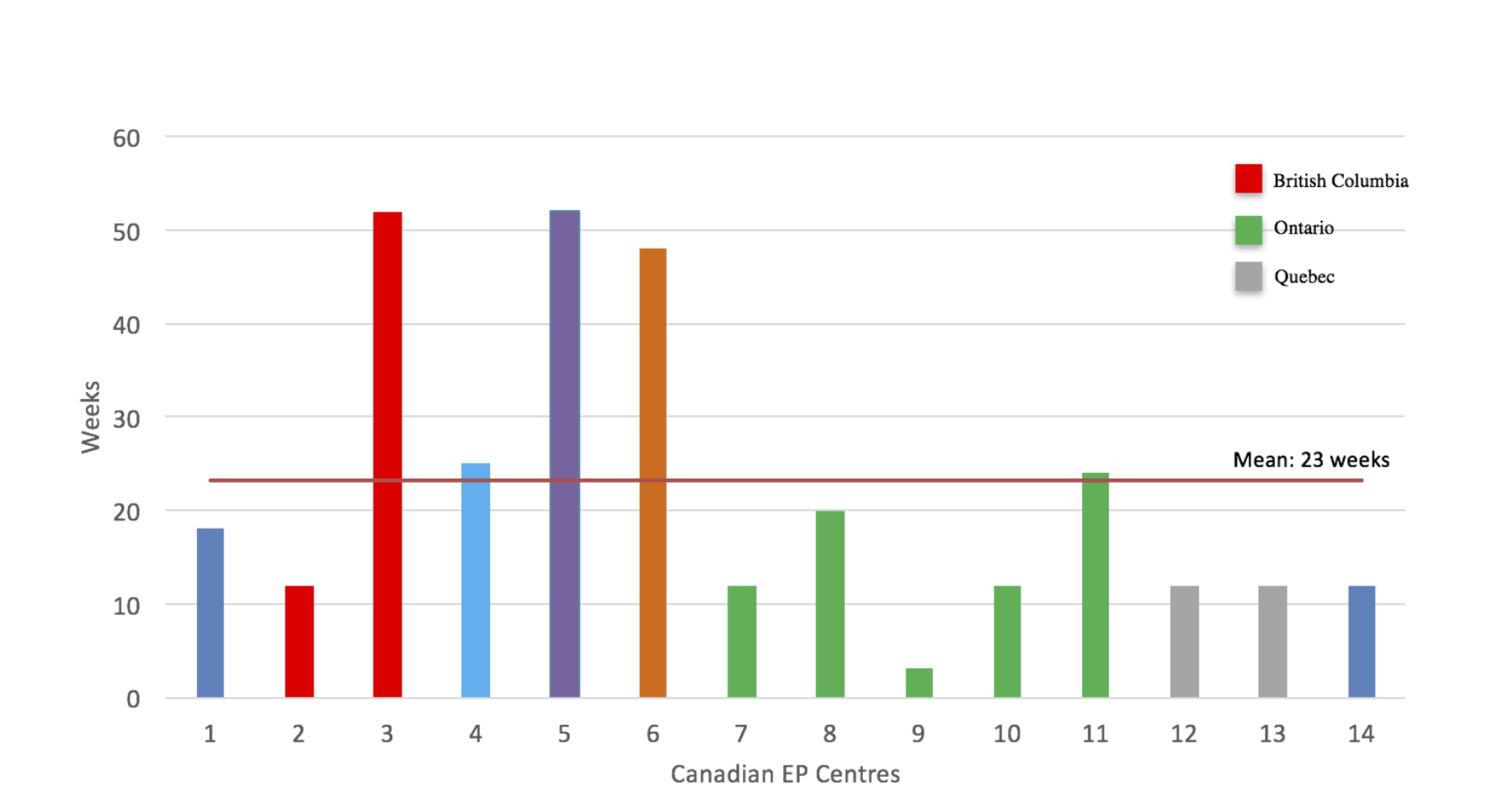
If we solely consider the 11 centres that contributed data from 2011, the total number of ablation procedures increased from 4908 in 2011–2012 to 5478 in 2015–2016; with an average of 498 ± 298 versus 446 ± 237 ablations. Figure 1 depicts the trends of the annual number of ablation procedures performed in these eleven centres.
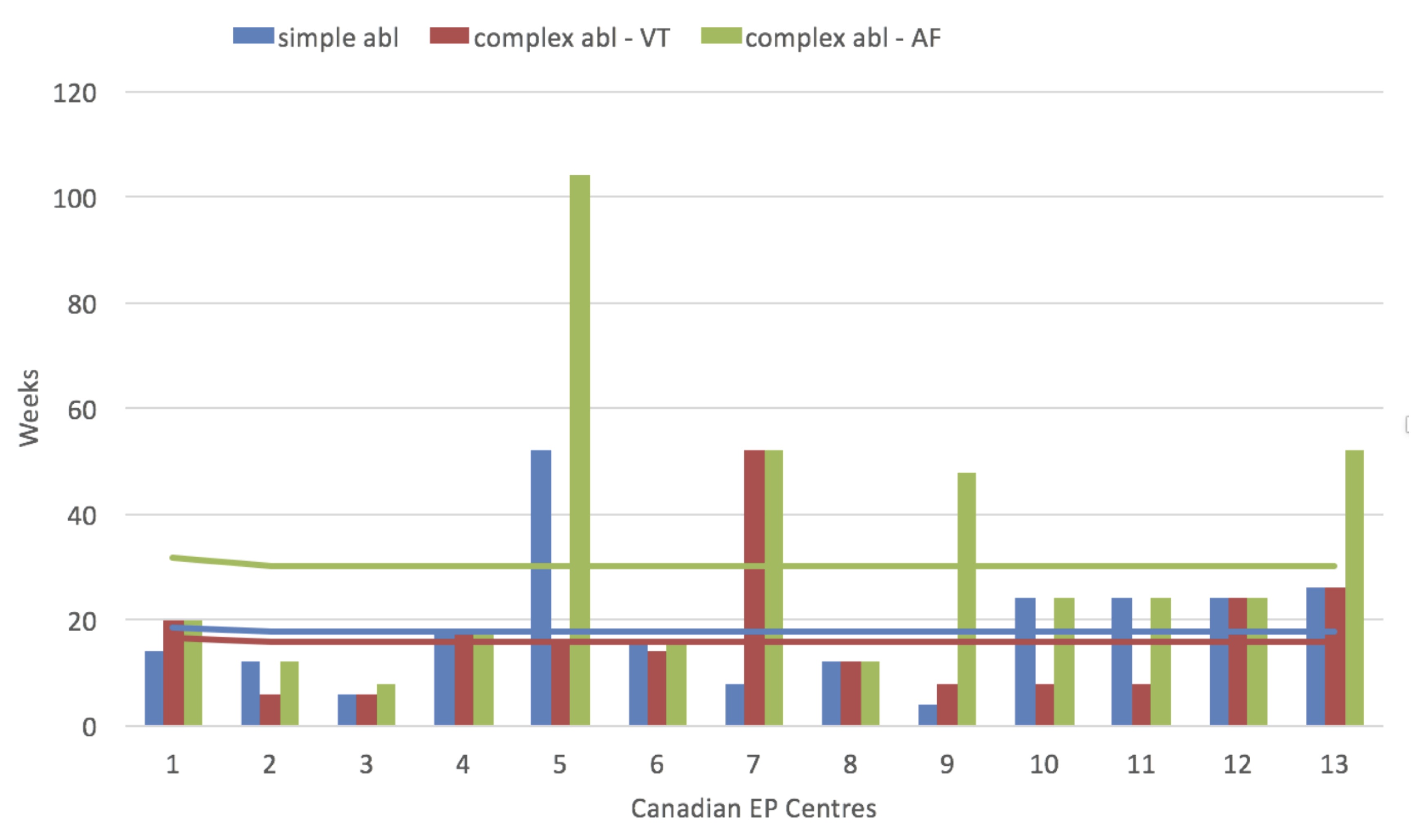
On average, each EP specialist was found to perform 117 ± 70 ablations annually in 2015–2016, increased from 113 ± 42 procedures in 2011–2012; part-time physicians were assumed to perform one half of the ablation volume of full-timers. Figure 2 depicts ablations done per operator.
Ablation results by substrates
Substrate-specific data were available from eight centres from 2016, seven centres from 2015; six centres in 2014, five centres in 2013, thirteen centres in 2012, and seven centres in 2011. This comprised a total of 18,864 ablation procedures that were performed over the 6 years (2011–2016), and were included in the following substrate specific analysis. The most frequently performed ablation was targeting AF (PVI) arrhythmia accounting for 36% of all procedures in 2015-16 (n = 2945, mean = 164 ± 85, range = 54–333), 32% for the years 2013-4 and 30% in 2011-2. Paroxysmal AF decreased from accounting for the majority (93%) of all AF ablations in 2012 to 55% of the cases in 2016, contrary to persistent AF which increased from 29–47%. Chronic success remains consistently > 70% for paroxysmal AF procedures, and varies between 60%-90% for persistent AF.
The second common procedure was the ablation of atrioventricular node reentry tachycardia (AVNRT) accounting for 18% of all procedures in 2015–2016 (n = 1489), which has decreased from 2011 when this dysrhythmia comprised 23% of all ablated substrates. The total number of cavotricuspid isthmus (CTI) ablations in 2015-16 was 1473 averaging 98 ± 71 ablation procedures per centre (range 37–327), comprising 17% of total volume of ablations. Ablation of Atrioventricular Junction and ventricular tachyarrhythmias were the most rarely performed ablations. In 2015–2016 they accounted for 7% and 8% of ablations respectively, and 8% and 7% in 2013 and 2014. Table 3 shows the relative frequency of different ablation targets treated by catheter ablation in all centres.
Table 3
Volume of Ablation procedures by substrate 2011–2016 reported as percentage of total respondents.
| |
2015–2016
|
2013–2014
|
2011–2012
|
|
Atrial Fibrillation/Atypical Flutter
|
36%
|
32%
|
30%
|
|
AV Nodal Re-entry Tachycardia
|
18%
|
22%
|
23%
|
|
Typical flutter
|
17%
|
16%
|
21%
|
|
AV Reciprocal Tachycardia
|
10%
|
10%
|
11%
|
|
Atrial Tachycardia
|
3%
|
4%
|
6%
|
|
Atrioventricular Junction
|
7%
|
8%
|
n/a
|
|
Ventricular Tachycardia
|
8%
|
7%
|
9%
|
|
Total annual ablations in 11 consistently respondent centres
|
5478
|
5243
|
4908
|
| AV = atrioventricular |
Procedural complication rates and success rates
Major complications from ablation of accessory pathways (AVRT), AVNRT, and CTI include pericarditis, transient PR prolongation, tamponade, pericardial effusion, stroke, indication for a permanent pacemaker, vascular complications requiring intervention, and death. Minor complications were defined as vascular, hematuria, arteriovenous fistula, pseudoaneurysm, and pain during procedure. The following are self-reported procedural complication and success rates for the 2015–2016 survey. The rate of both major and minor post-procedural complications for the aforementioned substrates were reported as < 10% in 6 of 7 centres that provided complication rate data, and < 1% in 1 of the centres. Two centres reported pulmonary embolisms post procedures. The chronic success rate, defined as ‘no recurrence or palpitations were documented other than target arrhythmia’ was greater than 90% in most (80%) of reporting centres. Partial success, defined as ‘recurrence with episodes of lesser frequency and severity, requiring the patient to be on the same medications’, occurred with < 10% frequency in 2 centres, greater than 90% frequency in 2 centres, and 10–20% in the remaining centre.
Ablation of AF most commonly leads to minor complications that requires a hospital stay of > 24 hours and other complications that don’t require intervention: vascular complications, hematuria, arteriovenous fistula, pseudoaneurysm, and groin pain. Six of 7 centres that reported complications in 2015–2016 had a < 10% minor complication rate, and one centre reported a < 1% incidence of minor complications. Major complications of AF: vascular complications requiring intervention more specifically pericarditis, tamponade, pericardial effusion, stroke, need for permanent PM, atrio-esophageal fistula, death, occurred with the same frequency. Chronic success of AF as well as CTI/MAT/FAT ablations were defined as ‘no recurrence or documentation other than target arrhythmia’, it was > 80% in 2 centres, 71–80% in 1 centre, > 90% in 1 centre, and 1 centre reported a 61–70% rate for 2015–2016. Partial success was < 10% in 2 centres, 21–30%, 71–80%, and > 90% in 1 centre each.
Ablation of Ventricular Tachycardia had similar major complication rates. Five out of seven centres reported < 10% minor complication rates, 1 centre reported a < 1% rate, and in one centre 10–20% of procedures yielded minor vascular complications of AV fistula and pseudoaneurysm not requiring intervention.
Post procedural care
In 75% of polled centres reported that patients are discharged > 24 hours post AF ablation procedure, and in 25% centres patients are discharged same day. Those undergoing RVOT ablations 50% were discharged same day, and 50% >24 hours post ablation. In AVRT/AVNRT/CTI ablations 75% of patients are discharged same day, and 25% in > 24 hours.
Ablation of Atrial Fibrillation
Paroxysmal AF was more common than persistent and permanent AF. Paroxysmal AF made up 55% of annual AF cases in 2016, and made up the majority (93%) of annual AF cases in 2013. Chronic success, defined as ‘12 months free from documented AF of 30 seconds or more’, was achieved after about 70% of ablations of paroxysmal AF, ranging from 69%-71% between 2013 and 2016. Chronic success was achieved for a range from 60–90% of non-paroxysmal AF ablations. Cases had to be redone between 15–22% of paroxysmal AF, and between 17% and 28% of non-paroxysmal AF ablations. Table 4 presents the volume of cases and complete technological data as it pertains to PVI procedures.
Table 4
Procedural and infrastructure data as it pertains to ablation of Atrial Fibrillation arrhythmia.
| |
2016
|
2015
|
2014
|
2013
|
|
Paroxysmal AF
|
55*
|
58*
|
84*
|
93*
|
|
Redo cases
|
22%
|
15%
|
15%
|
22%
|
|
Chronic success
|
71%
|
71%
|
69%
|
69%
|
|
Non-Paroxysmal AF
|
47*
|
42*
|
34*
|
29*
|
|
Redo cases
|
17%
|
22%
|
21%
|
28%
|
|
Chronic success
|
60%
|
62%
|
90%
|
85%
|
|
Modality
|
|
|
|
|
|
Manual
|
100%
|
100%
|
100%
|
100%
|
|
STXS
|
17%
|
13%
|
17%
|
17%
|
|
NMARQ (RF)
|
17%
|
13%
|
0%
|
0%
|
|
Ablation Hardware Availability
|
|
|
|
|
RF irrigated
|
100%
|
100%
|
100%
|
100%
|
|
RF non-irrigated
|
33%
|
25%
|
0%
|
0%
|
|
Cryoballoon
|
100%
|
88%
|
33%
|
33%
|
|
Arctic Front
|
100%
|
75%
|
44%
|
33%
|
|
Contact Force
|
100%
|
100%
|
n/a
|
n/a
|
|
PVAC
|
17%
|
25%
|
22%
|
33%
|
| * average annual procedures per year |
In 2016, PVI procedures were done under general anesthesia ‘rarely’ in 50% of the centres, ‘most of the time’ in 33% of the centres, and used for ‘all’ the cases in 17% of the centres. Conversely, 50% use non-general anesthesia most of the time, 38% use it rarely, and 13% don’t use it at all. During the years 2014 and 2013, 25% of the centres used general anesthesia in half of atrial fibrillation ablation cases; 63% of the centres performed most of the cases under general anesthesia and 13% of the centres rarely used general anesthesia. Meanwhile, 25% of the cases used non-general anesthesia in half and most of the cases, and 50% of the centres only rarely used non-general anesthesia.
Finally, the questionnaire evaluated the type of imaging that was done prior to AF ablation; five centres provided the data for the year 2016. Pre-procedural MRI or CT was done in 76–90% of the cases by 2 centres, and > 90% in 3 centres. Pre-procedural TEE was done in > 90% of the cases in 3 centres, 76–90% of the cases in 1 centre, and done 1–25% of the time in the remaining centre. In 2015, 40% centres conducted pre-procedural CT or MRI imaging on 76–90% of the cases, 60% on > 90% of the AF ablation cases. In both and 2013 and 2014, 75% centres conducted the pre-procedural CT or MRI imaging, while 13% did an MRI or CT on 76–90% of the cases and 13% of centres do an MRI or CT on less than 25% of the AF procedures.
{kind=link}
{kind=link}