While laser retinopexy is typically a safe procedure, complications may arise. Inadvertent laser to the macula, choroidal effusions (especially when large amounts of laser are used), angle closure glaucoma, ERM formation, anterior segment laser burns, hemorrhage (of the retina, vitreous, or choroid), choroidal neovascular membrane formation, and the formation of new retinal breaks are just a few examples. Iatrogrnic consequences include laser burns to the anterior segment and accidental laser to the macula [8].
Mester U, et al. studied retrospectively 2,000 eyes with retinal breaks and degenerations that had been treated with argon laser photocoagulation, with follow-up ranging from 6 to 84 months (mean 46 months). Only petectal intra- and preretinal hemorrhages occurred after photocoagulation, which resolved after a few days. Complications after treatment were limited to ERM formation in the macular area in four eyes (0.2%). Three of these four eyes had much more applied laser energy (mean 34.4 mJ) than the other 2,000 eyes (mean 7.2 mJ). They came to the conclusion that extensive photocoagulation is linked to an increased risk of ERM [9]. With the exception of one study that reported a significantly higher incidence of macular ERM formation, characterized as macular pucker, after laser treatment or cryoretinopexy (40 and 43%), previous studies showed a low (0 to 2.3%) incidence of macular ERM formation, after laser treatment or cryotherapy [6]. 205 eyes with retinal tears treated with laser retinopexy, cryoretinopexy, or both were reviewed retrospectively by Saran BR and colleagues (with minimum 6 months follow-up). 10 percent of eyes treated with cryoretinopexy, 14 percent of eyes treated with laser, and 18 percent of eyes treated with both cryoretinopexy and laser retinopexy developed an ERM. There was no statistically significant difference in the incidence of macular ERM across the treatment modalities. They found that the difference in ERM incidence in their research compared to prior studies might be due to changes in categorization, detection sensitivity, and degree of treatment [6]. Blackorby BL,et al evaluated retrospectively 2257 eyes with retinal tears treated with laser retinopexy, or cryoretinopexy. After treatment of retinal tears, 4.32 percent of cryoretinopexy eyes and 2.90 percent of laser retinopexy eyes had an ERM. The average time to ERM formation in their research was 11.5 months for cryoretinopexy and 12 months for laser retinopexy [1]. At the 6-month follow-up in our trial, none of the patients developed ERM. This outcome might be related to the fact that our research had fewer patients or a shorter follow-up period.
In patients treated with laser retinopexy, Khan Ashraf A and colleagues observed a 3.16 percent incidence of retinal detachment (RD). Early detachments (within 100 days of laser retinopexy) were caused by new or overlooked breaks in their study. In their investigation, the late RD was caused by the same treated retinal break. This finding might be owing to early undertreatment with sluggish advancement, or minor innocuous ocular trauma that progresses to RD via regions of weak retinal adhesion [10]. At the 6-month follow-up in our study, none of our patients developed RD.
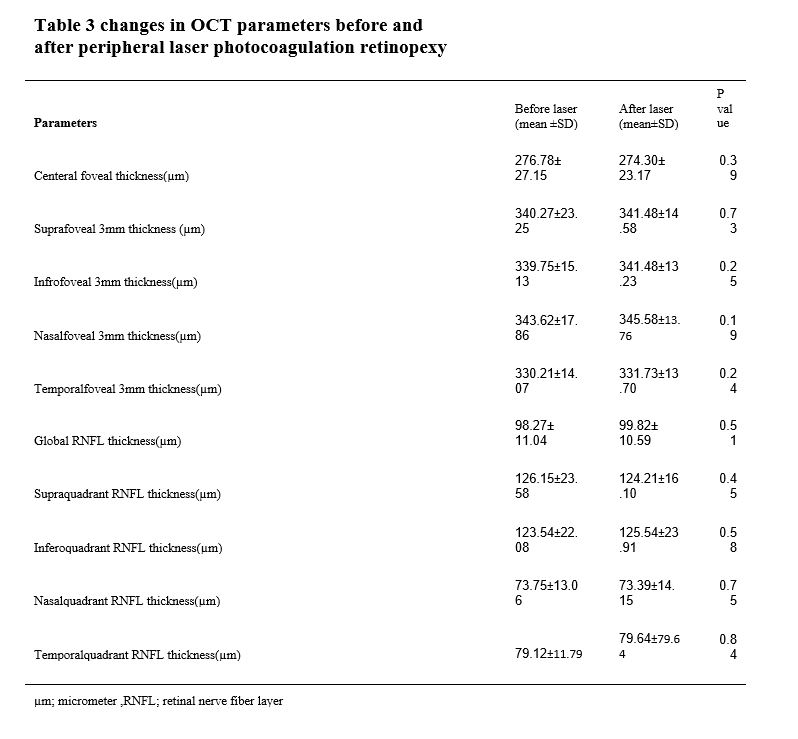
Only a few studies have looked at changes in macular OCT following laser retinopexy. In one research, 25 myopic eyes with peripheral lattice degenerations had their macular OCT alterations assessed following laser photocoagulation. They found that following laser photocoagulation, the vitreoretinal tractions were blunted in macular OCT [11]. Ours is the first prospective research to show changes in macular and retinal nerve fiber layer (RNFL) OCT following peripheral laser photocoagulation retinopexy (for retinal breaks, retinal holes, retinal dialysis, and lattice degenerations). After peripheral laser photocoagulation retinopexy, no statistically significant differences in macular and RNFL OCT values were identified.
There is no research on IOP variations following laser retinopexy in the literature. However, there have been some reports of alterations in IOP after panretinal laser photocoagulation (PRP). Increases in IOP of more than 6 mm Hg are prevalent after PRP, with 32 percent to 94 percent of patients seeing a rise in IOP of more than 6 mm Hg [12, 13]. In a research by Blondeau et al, all occurrences of PRP-related ocular hypertension were diagnosed within 2 hours after laser therapy [13]. No patients in our research had a rise in IOP throughout their follow-up.
This is the first prospective research to look at ERM development, microstructural alterations in the macular, and RNFL OCT in patients who had peripheral laser photocoagulation retinopexy. Nonetheless, there are several drawbacks to this research, such as the absence of a control group and the use of a non-randomized technique to recruit patients from a restricted number of medical institutions, which raises the risk of selection bias. Furthermore, we followed up with the patients for roughly 6 months, and longer follow-up periods may reveal a larger complication rate. More prospective clinical studies with larger sample numbers are required to assess microstructural changes in the macula and ONH, as well as to determine the incidence of macular ERM development and clinically significant macular pucker following laser retinopexy.
{kind=link}
{kind=link}
{kind=link}