Color perception predominantly relies upon human physiology which involves the cone-shaped receptor cells. The selection of the shade ideally is done within 5–7 seconds because cone receptors in the retina undergo fatigue and become sensitive to further stimulation. 222(41.8%) respondents prefer to select the shade within 5–7 seconds. Eyes do not fixate at a single spot but rather wander the optical field continuously, especially when you are presented with two adjacent areas with different colors, resulting in the formation of overlapping afterimages. To overcome this, break is given to the eyes by looking at neutral grey or blue backgrounds.[11] 378(71.3%) dentists prefer to observe at neutral grey or blue cards if time extends during shade matching. In this study, 283(91.1%) dentists prefer to take patients' opinions during shade analysis and it has been recommended to take patients' opinions whenever shade selection is being made.[11]
Precise color perception and shade analysis are achieved with a lighting intensity of 150–200 foot candles with a color temperature of 5500 kelvin.[12] Intensity and quality of light in the operative field can be evaluated using a light meter and a color temperature meter respectively.[11] The highest proportion of respondents 512(97.9%) felt natural daylight is the ideal source of light for shade analysis. Best color perception can be achieved with color corrected lighting tubes with D 55 illuminants which produce the closest depiction to the natural sunlight.[13] 409 (77.1%) dentists prefer to perform shade matching at 10 am to 2 pm which is the best time to perform shade matching. Use of dental chair light and incandescent bulbs is not recommended in the shade analysis because of a greater amount of yellow light eminence.[11]
Perception of color is affected by the surrounding environment including relative lightness, color, and saturation. Contrast effects are optical phenomena that can significantly modify color conception.[11] For best shade analysis, it is preferred to select the lighter shades for patients with lighter tones and vice versa to prevent the effects of value contrast effect.[14] In the present study, 437(82.4%) respondents felt that the surrounding environment have a profound effect during shade analysis. It has been recommended to remove the cosmetics that are applied on the lips, as they affect the perception of the color during shade analysis.
391(73.7%) participants prefer to maintain a distance of 25-35cm at the time of shade analysis. Tooth close to the viewer will appear larger and lighter and posterior teeth turn up darker. Hence, a 25 cm distance should be maintained from the patient's mouth to obtain a stable result.[11]
In the current study, 367(69.2%) respondents practice shade matching by placing the shade tabs adjacent to the tooth to be matched. When two objects are placed adjacent to each other with uniform illumination, a binocular color discrepancy occurs, i.e., one object turns up lighter than the adjacent object. During shade analysis, it is considered to placing the shade tabs either below or above the tooth to be matched, will helps to eradicate the binocular color discrepancy.[11]
246(46.4%) respondents prefer to delay the shade analysis for one week after bleaching. Bleaching results in dehydration, brightening, and removal of pigmented stains between the hydroxyapatite crystals, thereby decreasing translucency and increasing the opacity of the enamel. Hence, shade analysis should be postponed for at least one month after bleaching for rehydration of enamel and to restore translucency.[11]
180(33.9%) dentists felt that value is the most critical dimension for color perception in shade rendering. In the newly erupted teeth, the superficial enamel is highly reflective with high opacity and increased value. Underlying dentin which represents the chroma of the tooth will be lower due to the overlying young enamel. As the age increases, upper layers of the enamel are worn, the value decreases, and chroma increases due to the secondary dentin formation. Value is the important color rendering element and should be measured first.[11]
292(55.0%) respondents prefer to do the shade analysis before the initiation of treatment. Shade analysis must be done before you turn on the dental chair light and before initiation of treatment. Rods and cones in the retina of the eye are perceptive to light and result in eye weariness and glare.[11] 343(64.7%) dentists prefer to select the shade for each of the three distinguishing color zones gingival third, body, and incisal third. Color transitions in the surface change from one surface to another due to the difference in the thickness of enamel and dentin. To achieve the ideal color perception, the clinician must evaluate each of the three sections of the tooth, gingival, body, and incisal.[11]
217(40.9%) respondents are not following any isolation method during shade analysis. 213(40.1%) respondents chose cotton rolls, 19(3.5%) used Teflon tape for isolation during shade analysis and 81(15.2%) used rubber dam. The dark value of the rubber dam sheet will trick the eyes into recognizing the tooth shade as being lighter. The final shade of the restoration will be too dark in consonance with the adjacent tissues.[15] 232(43.7%) respondents prefer to dry the teeth while shade matching. Chroma and translucency decrease and value increases on dehydration of teeth. Shade analysis must be carried out after cleaning the debris and the teeth must be in moist condition.[16], [17]
Most of the participants in the current study preferred to use manual shade selection over digital shade selection. Similar observations were made by Dagg et al and Alruwaili et al.[18], [19]
206(38.8%) respondents felt that the shade tabs in the shade guide represent hue with increasing chroma within groups. 158(29.8%) respondents surmised that shade tabs represent hue with increasing chroma within groups or value. 56(10.5%) respondents felt that tabs in the shade guide illustrate only value. 110(20.7%) practitioners have no idea what the shade tabs in the shade guide depict. Generally, shade tabs are arranged according to the value from lightest representing high value to darkest delineating low value, hue, and chroma, depending on the design of the shade guide. Shade analysis is better executed in the order value, chroma, and hue.[11]
269(50.7%) practitioners prefer to use VITA Classical A1-D4®shade guide, 149(28.1%) practitioners use VITA System 3-D MASTER shade guides®, 32(6.0%) practitioners use VITA Linear guide 3-D MASTER® for shade analysis. 14(2.6%) respondents practice computer-assisted shade analysis. It is advantageous to use independent shade guides for composite and ceramic restorations. [20] 276(52.0%)respondents prefer to use separate shade guides for composite and ceramic restorations. 254(47.9%) respondents use the same shade guide for both composite and ceramic restorations.
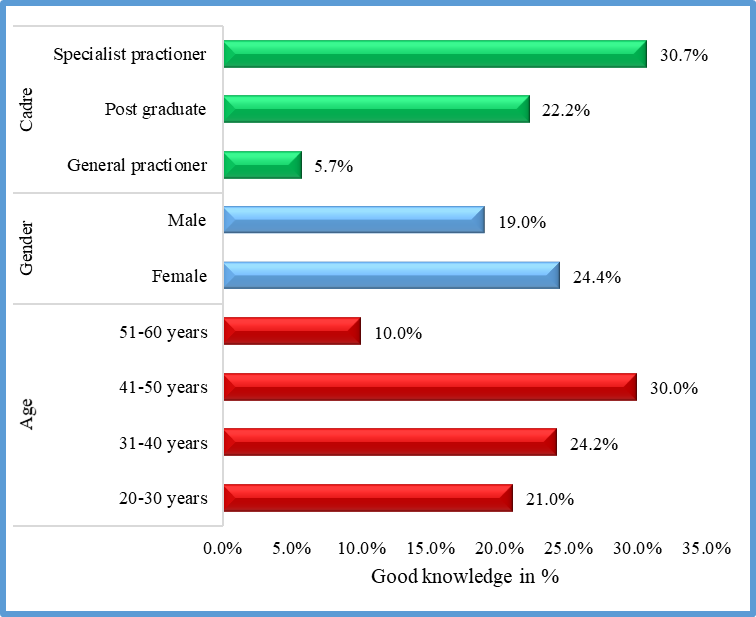
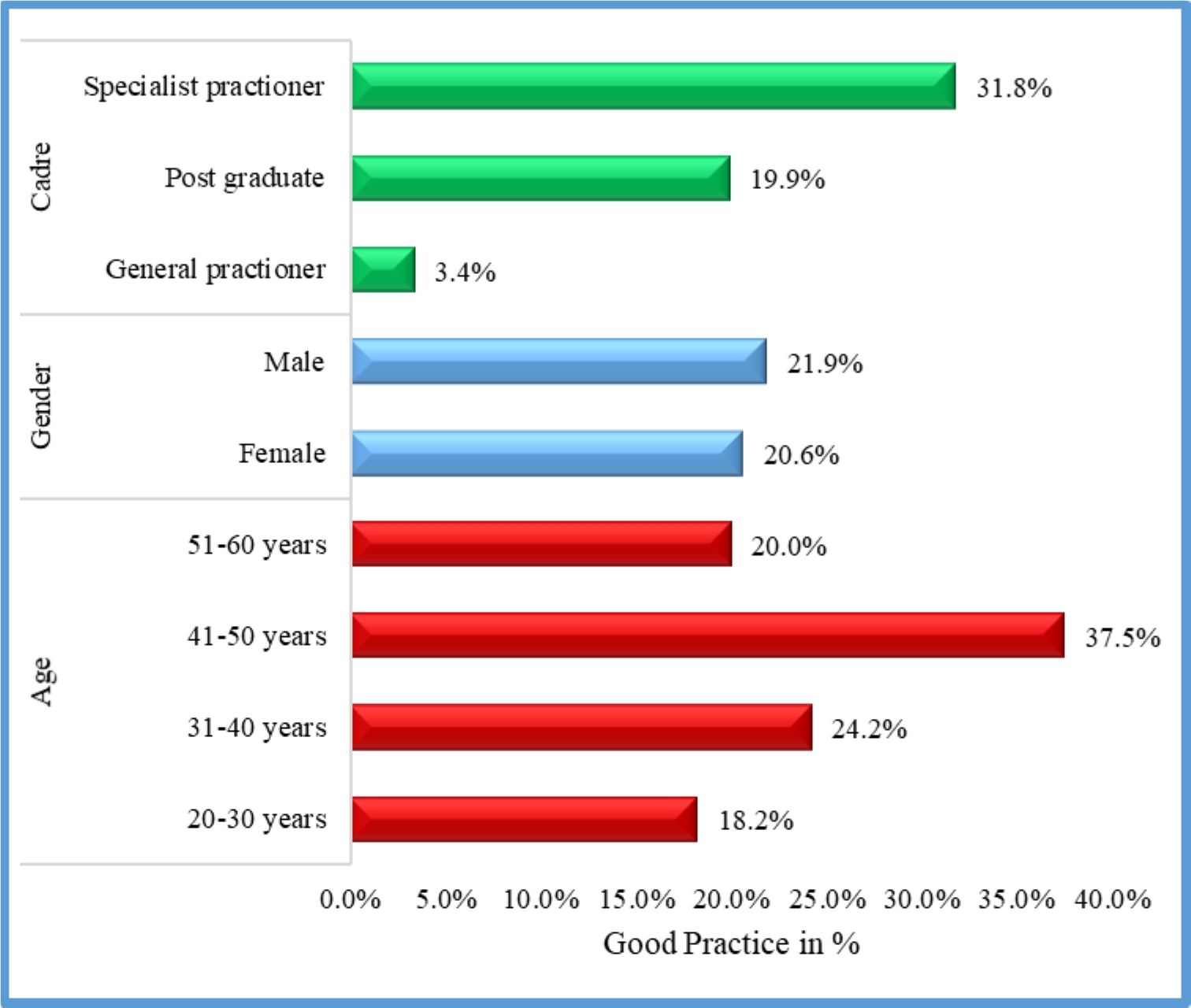
481(90.7%) respondents have shown interest to participate in the CDE program on esthetic restorations. 150(28.3%) members have not attended any CDE program. CDE programs play a pivotal role in understanding the potential factors affecting the perception of color and principles for shade analysis thereby allowing the dental practitioners to redeem for them to attain the accurate shade analysis.[21] Overall, specialist practitioners showed better knowledge and practice compared to postgraduates and general practitioners. This is in accordance with a study conducted among Nigerian dentists by Enone et al.[22]
{kind=link}
{kind=link}