The main findings of this study were the incidence and prognostic value of the lung metastasis of TC compared with that of other site-specific metastases. This will help us to have a better-informed discussion with the patients concerned and help us understand the overall prospect of the disease. Moreover, survival data about whether surgical treatment of the primary or distant LN(s) or other metastatic site(s) is beneficial for TC lung metastasis and other organ metastases will help us make more appropriate clinical decisions about TC.
In our analysis, we found that white race patients had a survival advantage in terms of both overall survival and thyroid cancer-specific survival when lung metastases occurred. Referring to other studies [5, 6]. This may be explained by better social support, including Medicare. Some experts considered it an independent prognostic factor of recurrence and metastasis in thyroid cancers [7]. Regarding the intrinsic differences in tumor biology, genome and/or gene variation was also considered a possible explanation for the differences between races[8]. In addition, a small study using a microRNA expression profile reported that there were microRNA expression differences between races, which may also be related to the potential variation of tumors[9].
In this study, we found that lung metastasis from the thyroid was worse than bone metastasis, but it was still not as bad. In many kinds of cancer, bone metastasis generally has a relatively better prognosis[10] [11], but lung metastasis is not necessarily. Fortunately, as many other scholars have reported, pulmonary metastases may also have a better prognosis [4].
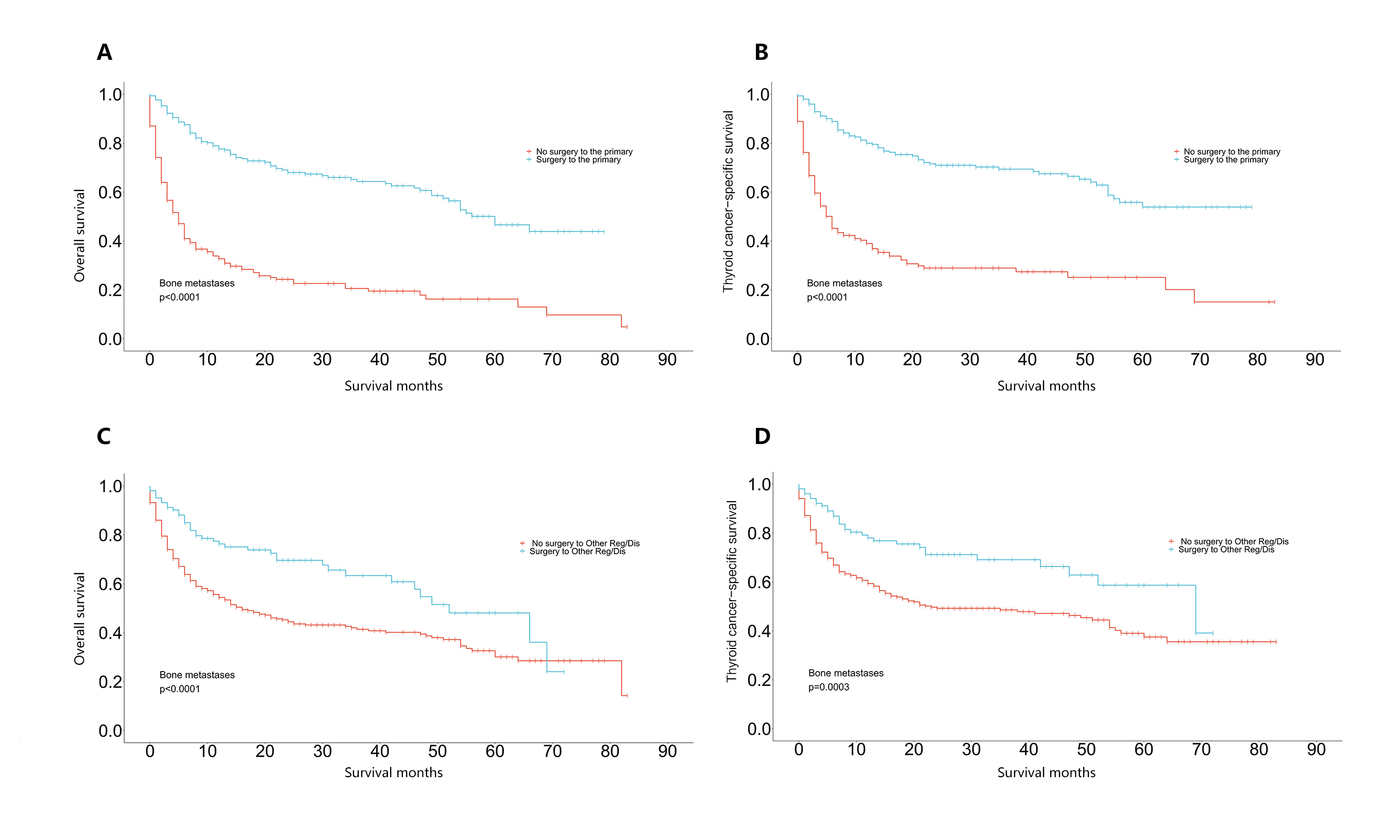
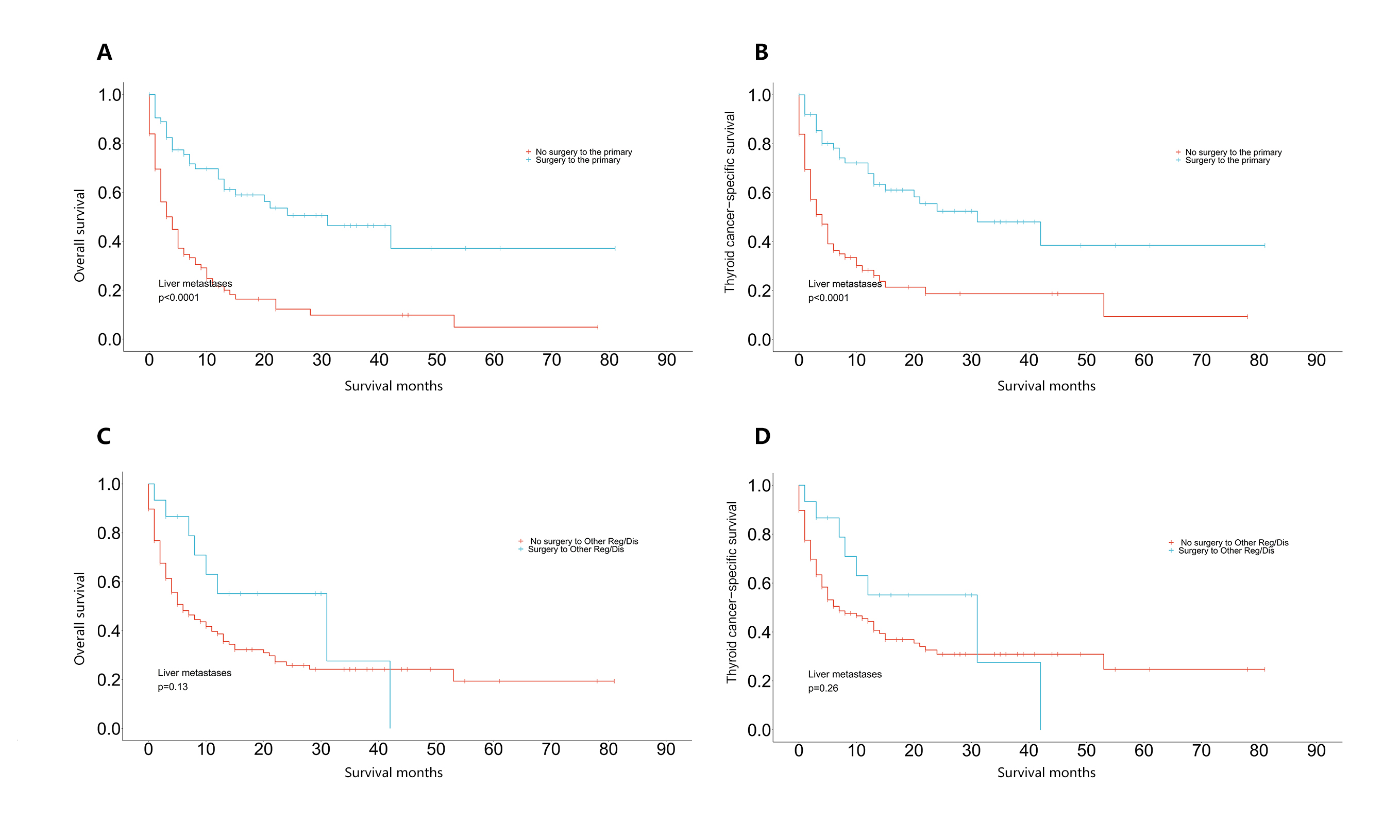
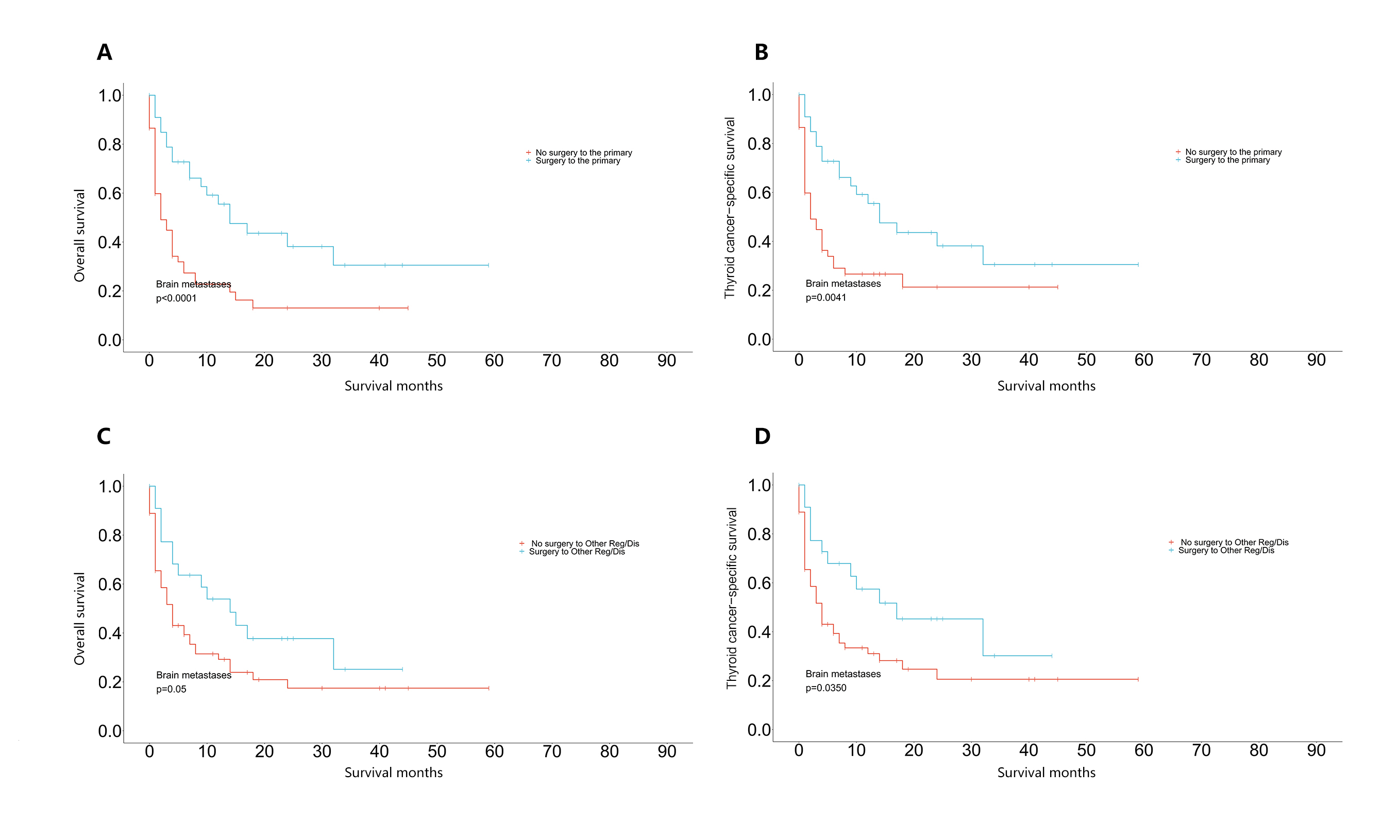
In our study, the prognostic advantage of surgery over a conservative approach for primary thyroid tumors was obvious among those with lung and other-organ metastases. However, for the treatment of metastatic sites, different strategies should be adopted for different locations of metastasis from the thyroid. Our studies have shown that patients with lung and bone metastases can benefit from surgical treatment of distant LN(s) or other metastatic site(s) in terms of both overall survival and disease-specific survival. This is similar to the general strategy for other metastatic cancers with better prognosis; that is, surgery for distant lesions may improve the prognosis[12] [13]. An important landmark publication is the 1997 report from Europe and North America, which indicated that the fewer the metastases and the longer the interval before their appearance, the longer the survival after metastasectomy[12] [13]. This implied that tumors with a relatively good prognosis may have a longer postoperative survival for metastasectomy. This may be an encouraging inference for surgical management.
Notably, except for surgical information, other related treatment information was incomplete in the SEER database. The multivariate analysis of this study revealed that surgery, as an important part of treatment, played a significant role in the outcomes of metastatic TC, especially for lung metastasis and bone metastasis. This reveals that we should be active in the treatment of TC metastases.
Other studies have reported a propinquity trend that multiple-site metastases were associated with an increased risk of death[4]. However, after comparing the survival data of isolated lung metastasis with those of multiple-organ metastasis, including lung metastasis, a phenomenon was revealed: the prognosis of isolated lung metastasis from TC was similar to that of lung-bone metastasis from TC; conversely, there was a significant difference between the prognosis of isolated lung metastasis and other multiple-organ metastases, including lung metastasis (>=3 organs). The cooccurrence of two metastatic lesions with a relatively good prognosis did not change the prognosis.
However, we have to consider the inherent difficulties of SEER database analysis, and the above results in particular should be cautiously interpreted. Therefore, prospective controlled studies are expected to evaluate the prognosis of patients, which could avoid many interference factors and allow further analysis. This work would take a long time to accumulate enough cases. Multicenter clinical studies or large-scale databases with more details may help us.
{kind=link}
{kind=link}
{kind=link}