The FFSFT is an uncommon variant of SFT and is composed of typical or cellular SFT with mature adipose tissues. Nielsen et al reported three cases, composed of hemangiopericytomas and adipose tissues in 1995 and referred to them as lipomatous hemangiopericytoma for the first time [29]. Guillou et al reported that lipomatous hemangiopericytoma shared the similar clinical course, pathological features, ultrastructural features and IHC staining with SFT, except for the presence of mature adipocytes [30].Therefore, the lipomatous hemangiopericytoma was regarded to be a subgroup of SFT. This tumor has been classified as a variant of SFT in the 4th World Health Organization (WHO) classification of Soft tissue and Bone Tumors. SFT is now reported in all anatomical sites, remaining a rare entity in the breast. But when it comes to FFSFT of the breast, no case has been reported in English literatures.
In the cases of breast SFT, including this case, except that a very small number of cases were accidentally found on routine mammography, most cases showed palpable masses of varying sizes, ranging from 0.6 cm to 10 cm with a mean of 3.29 cm and a median of 2.85 cm. Most of them were painless masses, and some cases were accompanied by pain [10, 20, 22]. Except that 8 cases did not mention the side, the side of breast involved in the reported cases was roughly similar, with 12 cases in the left and 12 cases in the right breast. The age of patients ranged from 38 to 88 years with a mean age of 61.6 and a median age of 62.5 years. There were 8 males and 24 females, male: female = 1:3, and the incidence rate of female was higher than that of male, but this discordant prevalence may be attributed to the judgment as to the epicenter of SFT [7]. The radiologic findings of SFTs are nonspecific [18]. Breast SFT often presents as a hypoechoic or inhomogeneous echoic hypervascular mass with benign features at the radiological work-up, such well-defined margins and smooth echostructure [5]. The elastography on US is not hard [2]. Breast SFT can be shown as a relatively well-defined mass without calcifications on mammography [8, 18]. While malignant solitary fibrous tumors (MSFTs) often present at least focal lobulated appearance [2, 5, 20], and it often be classified as BIRADS category 4C by radiologists [2, 5, 20].
Grossly, the surgical specimen consisted of a well-defined solidmass with clear boundary. The cut surface of the tumor was gray-yellow, and often without bleeding and necrosis. In cases of breast MSFT, focal invasive margins can sometimes be seen [5, 8, 20]. As with SFTs from other anatomic locations, Breast SFTs are characterized by a well-defined mass composed of bland oval to spindle cells arranged in a haphazard “patternless” pattern, alternating with hypercellular and hypocellular areas. Sometimes tumor cells are arranged in sheet-like, storiform, fascicular, and even a herringbone patterns. In the hypocellular areas, there is a characteristic hemangiopericytic vascular pattern, the so-called “staghorn” vessels, in a rich, collagenous stroma with ropy collagen. However, non-classical SFT have also been documented, such as SFT with extramedullary hematopoiesis (EMH) [31]. Breast MSFT is extremely rare, and only 4 cases have been reported so far. In addition to the morphological characteristics of classical SFT, the reported 4 cases showed mild to moderate cytological atypia and high mitotic activity(≥ 4/10HPFs) [2.5,8,20]. Of which, 3 cases showed infiltrative margins at least in the local area [5, 8, 20] and 2 cases were significantly hypercellular and showed tumor necrosis [5, 20]. In only one case, the diameter of the tumor was greater than 5 cm [20]. As the histological diagnostic criteria of MSFT are not very clear, so the diagnosis of MSFT requires a comprehensive evaluation based on the morphological criteria proposed, rather than making the diagnosis only according to a single index such as mitotic activity.
As to our case, in addition to the typical morphological characteristics of SFT, there were some mature adipocytes in the tumor tissue. The morphological characteristics were consistent with the FFSFT reported in the literatures. Although there was no pleomorphic and necrosis, the tumor was hypercellular and the tumor cells had mild atypia. In addition, the mitoses in the hot spot reached 4/10HPFs. Therefore, it presented some atypical characteristics in morphology. However, our case did not meet most of the histological diagnostic criteria of MSFT, so it could not be diagnosed as MSFT.
A combination of CD34, CD99 and Bcl-2 has been widely used to diagnose SFT. Although these IHC markers are highly sensitive and usually show diffuse and strong expression in approximately 90% cases, whereas the specificity of both these markers is low [1]. Since a wide variety of mesenchymal tumors can express these markers, especially when the tumor and SFT show overlap in morphological changes, the value of these markers in differential diagnosis has great limitations. In recent years, fusion genes of NAB2-STAT6 has been identified as a hallmark of SFT, and IHC staining shows that the diffuse nuclear expression of STAT6 is highly consistent with the fusion of NAB2-STAT6 gene. The diffuse nuclear expression of STAT6 is highly sensitive (97% − 100%) and specific (97.5% − 100%) for the diagnosis of SFT [1, 32]. It should be noted that the expression of STAT6 is generally reduced or not expressed in dedifferentiated SFTs [33]. However, in a few cases, STAT6 expression also occurs in other non SFTs [1]. In particular, this marker can be expressed in a small subset of well-differentiated liposarcomas (WDLPSs)/dedifferentiated liposarcomas (DDLPSs), which is usually focal positive [1, 32, 34]. This phenomenon is considered to be the over-expression caused by STAT6 gene amplification [34], while other CD34 positive or negative spindle cell tumors that need to be differentiated from SFT have no positive STAT6 nuclear expression.
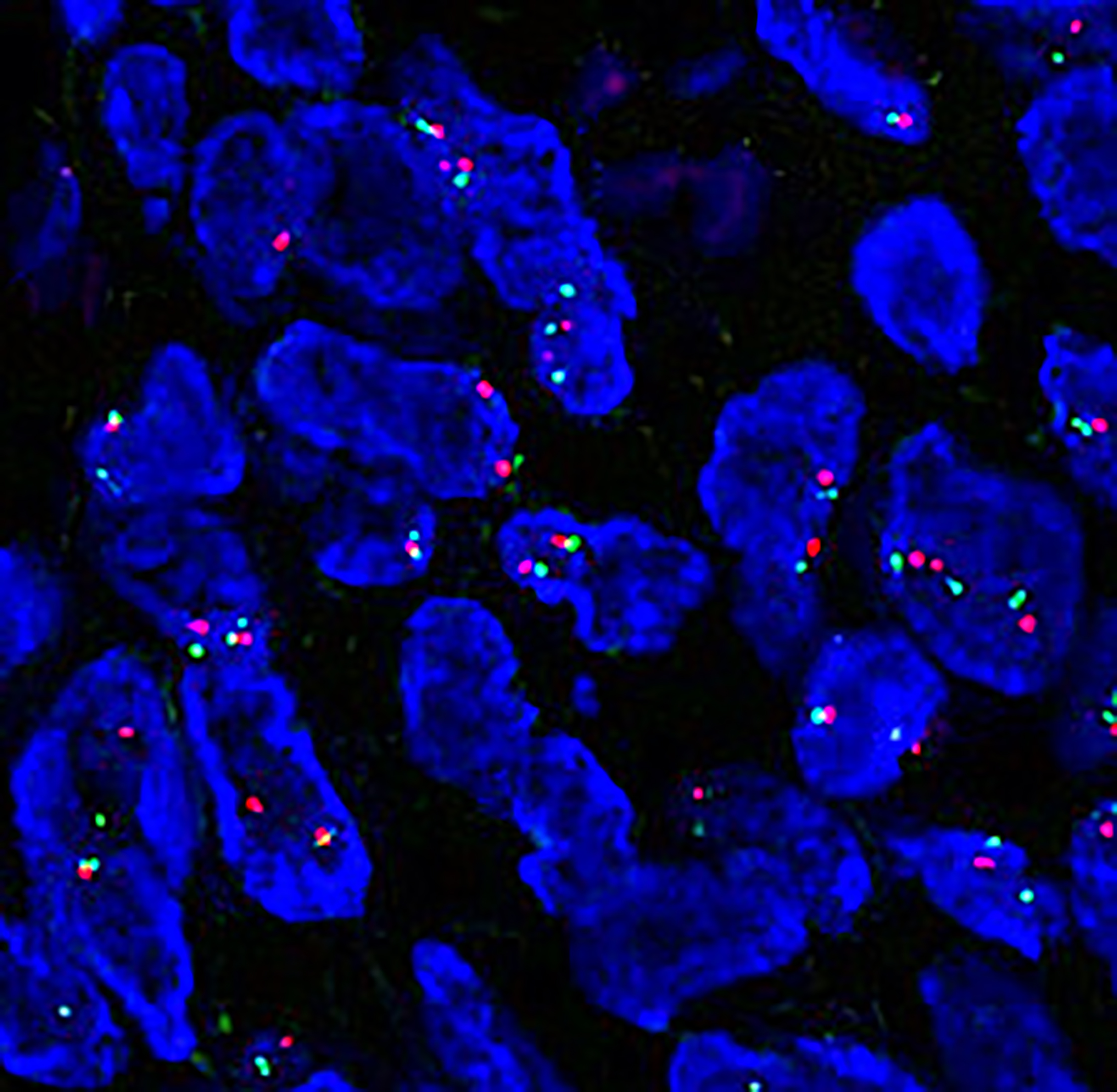
The adipocytic component of the FFSFTs reported in the literatures was mostly mature adipocytes [1, 35, 36], as showed in our case. Of note, multivacuolated lipoblasts and/or atypical lipomatous tumor-like areas can be observed in some cases, closely mimicking WDLPS [35]. In our case, no MDM2 gene amplification was found, and the NAB2exon6‐STAT6exon2 fusion gene transcript was detected by NGS, which confirmed that this case was FFSFT rather than liposarcoma. There are few previous studies on STAT6 IHC staining in FFSFT. Yoshida et al reported the expression of STAT6 in 49 cases of SFT, of which only 1 case was FFSFT. STAT6 was expressed in spindle tumor cells, and negative in adipocytes [32]. Creytens et al. evaluated the expression of STAT6 in 6 cases of FFSFT, and spindle tumor cells in 6 cases were diffusely moderately to strongly positive for STAT6 [36], but their article did not mention whether adipocytes expressed STAT6. Florian found that spindle cells in FFSFTs expressed STAT6, and some adipocytes also expressed STAT6 [37]. In this case, STAT6 IHC staining showed that the spindle cells and adipocytes in the tumor were positive, some adipocytes expressed S100, and a small number of adipocytes co-expressed STAT6 and S100, which indicates adipogenesis due to tumor differentiation rather than fat deposition due to degeneration. The interaction of STAT6 with genes regulating adipocyte differentiation, such as peroxisome proliferator activated receptor-γ(PPARγ), may provide a possible explanation for inducing adipocyte differentiation in FFSFT [37].
The differential diagnosis of breast FFSFT mainly include phylloides tumor (PT), myofibroblastoma, spindle cell lipoma (SCL), ASLT and DDLPS. ①PT is composed of epithelium and stroma. The stroma can have adipose components and adipoblasts, but the proliferative fibrous stroma often compresses the epithelium into fissures, and the fibrous stroma often expresses SMA and desmin, while SFT has no epithelial component and often does not express SMA and desmin. ②myofibroblastoma is circumscribed tumor composed of intersecting fascicles of bland spindle shaped myofibroblastic cells with intervening collagen bundles and mature adipocytes in different proportions. It often occurs in the breast and its morphology can be similar to FFSFT, but it always lacks the change of cell density and hemangiopericytoma like growth pattern. Although tumor cells demonstrate variable expression of CD34, Bcl-2 and CD99, but desmin and actin are always positive. This tumor is characterized by 13q14 and 16q deletion, resulting in partial or complete inactivation of RB1 and FoxO1 genes and subsequent loss of RB1 protein expression. Therefore, about 90% of myofibroblastomas shows loss of nuclear expression of RB1 protein. ③SCL often occurs in the head and neck dermis or subcutaneous tissue. It often has a complete capsule and exhibits bland spindle cells, ropy collagen bundles and mature adipose tissue and expresses CD34 immunostain [1]. This tumor also has RB1 gene deletion, resulting in the loss of RB1 protein expression.④ASLT is common in adults and has a wide incidence site, with more than half of it located in the limbs or extremities. Most of the manifestations are slow growing masses or bulges under the skin or fascia. The tumor often has no capsule, and about 35% of it can infiltrate the surrounding tissue. Histologically, ASLT consists of different numbers and proportions of atypical spindle cells and adipocytes including adipoblasts at different stages of differentiation distributed in mucoid and fibrous stroma. In most cases, singular multinucleated giant cells can be seen scattered. It often expresses S100, CD34 and desmin in varying degrees, but does not express STAT6, SMA, MDM2 and CDK4; About 57% of the cases shows loss of RB1 expression, which can be identified.⑤DDLPS exhibit a wide variety of histological features which resemble low- and high-grade sarcomas. It can resemble malignant FFSFT [1], In addition, another pitfall is that 11%-14% of DDLPSs can partially show STAT6 nuclear expression [1, 32, 34]. Notwithstanding immature adipoblasts are commom seen in DDLPS. In addition, the positive expression for MDM2, CDK4 and p16 IHC stains and the amplification of MDM2 gene detected by FISH helps in establishing the diagnosis of DDLPS [1].
Due to their rarity and lack of randomized control trials, there is no global consensus on treatment of breast SFTs. Complete excision with clear margins, a long-term follow-up and a multidisciplinary team approach are therefore recommended for treatment and management of these cases because of the unpredictable clinical behavior in some cases without malignant morphological features. Although our case showed the increased mitotic activity, but lacked other malignant histological features and the risk of metastasis was low. Therefore, adjuvant therapy was not given because there was no evidence that radiotherapy or chemotherapy did not actually increase any benefits. The patient was instructed to attend regular controls every 3 months. There was no recurrence and metastasis after 3 months of follow-up. The patient is still being followed up.
{kind=link}