Clinical characteristics of the study population
During the study period, 736 patients were evaluated for suspected AD, and 534 patients were enrolled in the study. Among the 534 patients (mean age 65.2±14.6 years, 69.2% males), 198 (37.1%) had a final diagnosis of AD; among these patients, 122 (61.6%) patients had type A AD, and 75 (37.8%) patients had type B AD.
Of the 336 (62.9%) patients in whom AD was ruled out, 105 (31.3%) had acute coronary syndrome, 2 (0.6%) had pulmonary embolism, 140 (41.7%) had atypical chest pain, and 89 (26.5%) had other diagnoses. The clinical characteristics, past medical histories and prevalence of ADD risk markers in patients in the AD group and control group are presented in Table 1.
Female sex, high heart rate, histories of diabetes, ischemic heart disease, and stroke were more frequently observed in the control group. Predisposing conditions and pain features were more often observed in patients with AD. However, pulse deficits were more frequently reported in the control group.
The distribution of time intervals between symptom onset and blood collection in these patients was also calculated and is shown in Table 2. A total of 32.3% of AD patients had blood drawn within 2 h of symptom onset, and a total of 77.7% of AD patients had blood drawn within 24 h. In contrast, 25.3% of non-AD patients had blood drawn within 2 h of symptom onset, and a total of 71.7% of AD patients had blood drawn within 24 h.
ADD risk score
The results of the ADD risk score are shown in Table 3. A low probability was observed in 65.6% of AD patients versus 75.0% of non-AD patients. In contrast, a high probability was more frequently observed in AD patients (34.3% vs. 25.0%, P=0.021).
Diagnostic performance of neutrophil counts
The sensitivity and specificity of neutrophil counts (cutoff: 6.2*109/L) in the general study population were 69.2% (95% confidence interval (CI) 62.2-75.4) and 56.0% (95% CI 50.5-61.3), respectively. The negative and positive predictive values (NPV/PPV) of neutrophil counts for AD were 75.5% and 48.1%, respectively, while the negative and positive likelihood ratios (NLR/PLR) of neutrophil counts were 0.55 and 1.57, respectively.
Because of the low sensitivity for AD diagnosis, further data analysis according to time intervals was performed. Figure 1 shows increased neutrophil counts in both the 2-8 hour (h) time interval and the 8-24 h time interval (both P<0.001), and there were no statistically significant differences between AD and control patients in other time intervals.
The sensitivity and specificity in the 2-8 h interval were 94.8% (95% CI 84.7-98.6) and 59.4% (95% CI 50.0-68.4), respectively, and similar sensitivity and specificity were observed in the 8-24 h interval group (96.9% and 45.0%, respectively) (Table 4).
Diagnostic value of the ADD risk score with neutrophil count
We combined the 2-8 h and 8-24 h groups into a new group (the 2-24 h group), with a sensitivity of 95.6% (95% CI 88.4-98.6), a specificity of 56.1% (95% CI 47.9-63.9), a NPV of 98.6%, a NPV of 55.5%, a NLR of 0.08, and a PLR of 2.71. Further analysis of the ADD risk scores was carried out in patients with data in the a 2-24 h time interval (Table 5).
The sensitivity and specificity of high probability (ADD>1) in patients in the 2-24 h interval were relatively low, 34.3% (94% CI 27.8-41.5) and 75.0% (95% CI 69.9-79.5), respectively. The sensitivity and specificity of neutrophil counts in low-probability patients were 94.6% (95% CI 84.2-98.6) and 52.3% (95% CI 42.1-61.9), respectively.
According to the ADD risk score, patients with AD who had either a low probability score or a high probability score showed significantly increased neutrophil levels compared to non-AD patients in the same risk group (Figure 2a).
The diagnostic value of neutrophil counts alone and neutrophil counts combined with the ADD risk score is presented in Table 5. The area under the curve (AUC) of the ROC analysis was 0.82 (95% CI 0.76-0.87, P<0.001) for neutrophil counts in all the 2-24 h interval study groups (Figure 2b, cutoff level of 6.2*109/L, with a sensitivity of 95.6% (95% CI 88.4-98.6), specificity of 56.1% (95% CI 47.9-63.9), NPV of 95.6% and failure rate of 4.3%). In the low probability group (Figure 2c), the AUC was 0.80 (95% CI 0.73-0.87, P<0.001, sensitivity of 94.6% (95% CI 84.2-98.6), specificity of 52.3% (95% CI 42.1-61.9), NPV of 95.0% and failure rate of 5.0%). In the high probability group (Figure 2d), the AUC was 0.84 (95% CI 0.77-0.92, p<0.001, sensitivity of 97.1% (95% CI 82.9-99.8), specificity of 62.5% (95% CI 47.3-75.7), NPV of 96.7% and failure rate of 3.3%).
Neutrophil count subanalyses according to the diagnosis of non-AD patients, type of dissection, and serial time interval change
Fig. 3 shows that the neutrophil counts in patients with AD were significantly higher than those in patients with acute coronary syndrome, atypical chest pain, or other diagnoses in the 2-24 h interval (neutrophil counts 11.7±5.4, 7.4±3.6, 6.3±2.9, 7.7±3.9, respectively). All P<0.001).
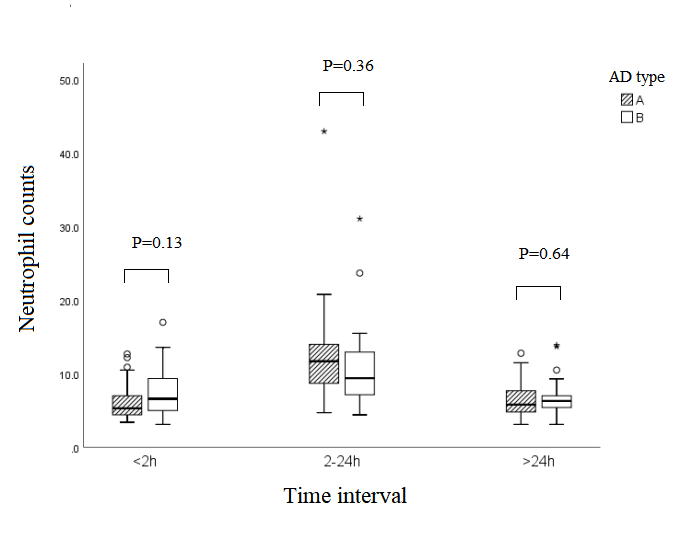
Neutrophil counts were also analyzed in patients with type A/B AD (Supplement Figure 1, Supplement Table 1). There was no significant difference in the neutrophil counts between patients with type A and B AD.
We further observed the trends in neutrophil counts among patients who had blood drawn multiple times to measure neutrophil counts. Twenty AD patients had neutrophil counts in both the 0-2 h and 2-24 h time intervals. The neutrophil counts increased from 6.4±3.4 (0-2 h) to 10.3±4.3 (2-24 h), with P<0.001 (Fig. 4).
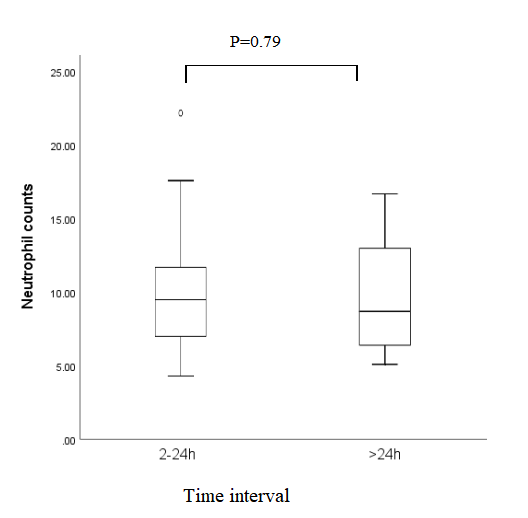
Another 25 patients with AD had neutrophil counts at both the 2-24 h and >24 h time intervals. These neutrophil counts were similar (9.9±4.1 vs. 9.7±3.5, P=0.79, Suppl. Fig. 2).
{kind=link}
{kind=link}