Study setting
EECC and ACC were costed for two low resource settings: Tanzania and Kenya. Tanzania and Kenya are both lower-middle-income countries in East Africa (GDP per capita: $1046-4095)(23) with decentralised health systems. In Tanzania the care referral system is organized in a pyramid structure, with the community centre at the base, followed by dispensary, health centres and district hospitals that constitute primary health care. These are followed by regional referral hospitals, zonal hospitals and specialized or national hospitals. While national policy has focussed on providing an essential health services package, problems have been identified with health care infrastructure, with many facilities lacking running water and telecommunications (24–26). In addition, facility surveys have found capacity for critical care to be limited, particularly at the district hospital level (15,27). In Kenya, the health system is also decentralised with resource allocation decisions devolved to the county level. Like Tanzania, the system also faces challenges in availability of resources including consumables, equipment and human resources at the facility level as well as regional disparities in availability of care with 22 out of 47 counties having at least one intensive care unit (28–30). We assume a setting where you cannot assume a constant electricity supply, but that care is being provided in a hospital, the patient has a bed, the patient is provided with other aspects of care and daily nutritional needs unless this forms part of critical illness care e.g. parenteral feed, the facility is cleaned and running water is available.
Intervention description
Critical care is the support of vital organ functions and complements the other care provided to a patient: the definitive care for the patient’s pathology (e.g. curative therapies such as drugs and surgery), hotel care (beds, sheets etc) and other care (e.g. psychosocial support) (see Figure 1).To provide effective coverage of EECC there are two core streams of activity: identification of the critically ill; and essential treatment of the critically ill(18). The identification stream involves the processes for identifying critical illness, distinct from the diagnosis of the underlying condition. The treatment stream is the organ support for a critically ill patient, including oxygen therapy, intravenous fluid resuscitation, and maintaining a free airway through correct positioning of unconscious patients.
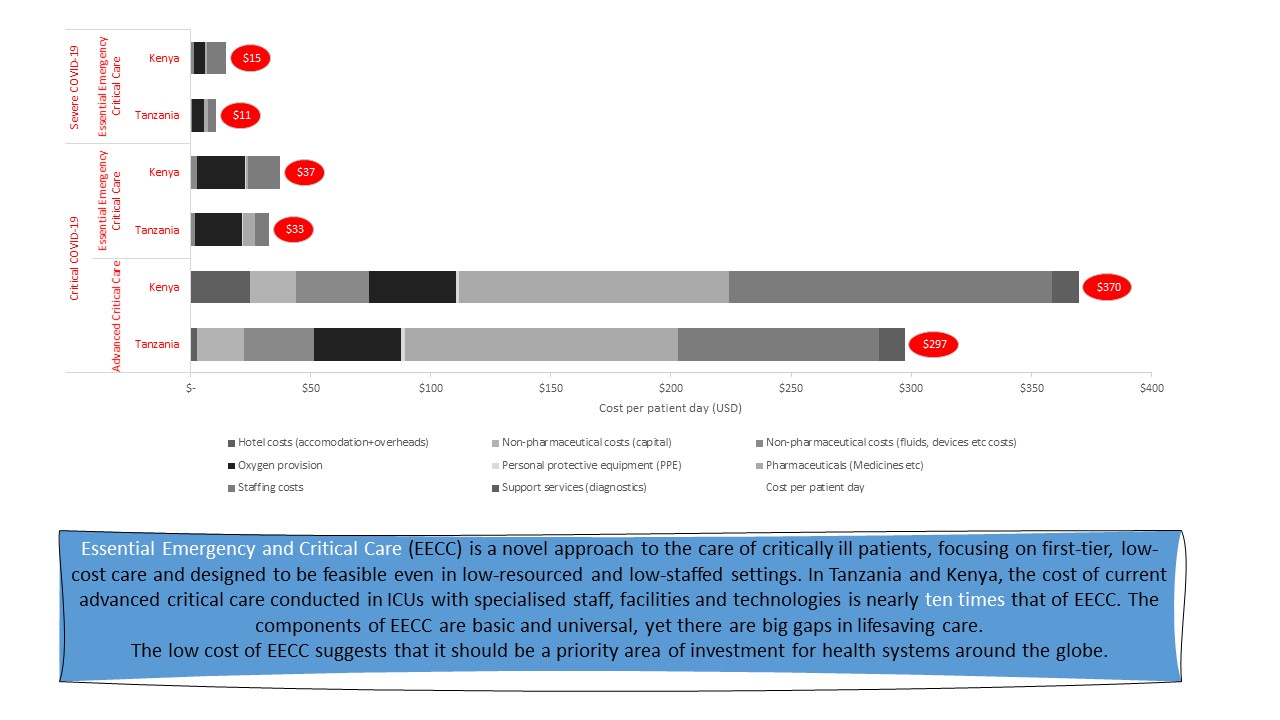
ACC was defined as the provision of EECC combined with the advanced resource-intensive care of critical illness typical of an ICU. A team consisting of Tanzanian and global critical care physicians with experience of the Tanzanian health system as well as other LMICs specified the content of ACC over and above EECC resources through documented current facilities and practices in the best resourced ICUs in Tanzania – care that includes mechanical ventilation and other advanced organ support, conducted with specialised staff, facilities and technologies.
Approach to costing
Identifying resources
The EECC Delphi consensus (17), was used to define all inputs required to provide EECC over and above the other care provided in the hospital setting (see Figure 1) and a list of inputs for ACC, excluding those required for EECC, was developed by the research team based on the intervention definition of advanced critical care (see Supplementary material 1). Both lists involved a set of equipment, consumables, drugs, human resources with staff trained to deliver care according to specific routines and guidelines. Costs were classified into the categories of Human Resources, Consumables (Pharmaceutical and non-pharmaceutical), Oxygen, PPE and Equipment. In costing EECC, we assumed a similar level of health facilities as a typical district hospital in Tanzania and a level 4 county hospital in Kenya. These characterizations informed the assumptions made around the specification of resource items.
Oxygen therapy is a core component of critical care for patients with COVID-19, as well as other conditions, and is a major portion of the cost (22,31). Oxygen therapy can be provided in different ways, depending on the needs of the patient and the setting or access to resources. We specified two different oxygen scenarios for EECC in the district hospital setting: (1) oxygen concentrators with cylinders as back up; (2) oxygen cylinders; and (3) one further scenario for higher flow oxygen in the ICU for ACC.
Quantifying resource use
Care for the critically ill varies according to the patient’s diagnosis and the severity of their critical illness. This heterogeneity means that an accurate quantification of resource use for all critically ill patients would require a large sample of patient observations. In the absence of such data, we selected COVID-19 as a tracer condition. We estimated treatment costs for COVID-19 patients in three separate severity categories – moderate, severe, and critical, based on WHO definitions (32). According to these definitions, patients with both severe and critical COVID-19 have vital organ dysfunctions and are therefore “critically ill” (20). Patients with moderate COVID-19 are not critically ill and therefore resources are only used within the identification stream for EECC and are not included in the ACC costing. For patients with severe COVID-19, resources are used within the identification and treatment streams of EECC. For ACC, severe patients are assumed to receive treatment and identification procedures as for EECC plus additional resources in the identification stream. For patients with critical COVID-19, resources included are across the identification and treatment streams for both EECC and ACC.
Resource use of the items specified in the input categories was quantified based on expert opinion. Clinicians on the research team, experienced in care of critically ill COVID patients, were asked to estimate the average resource use per patient per day of each included item for patients with moderate, severe and critical COVID-19. Two physicians provided estimates independently, the estimates were compared, and the physicians then discussed and resolved their differences to generate an agreed estimate.
Valuing resource use
All resources were costed at current (2020) prices to generate economic costs. Where possible local prices were sought. Capital costs were annualized using a discount rate of 3% as standard. All costs were converted to USD where necessary using current exchange rates (1 USD = 2300TZS, 115 KSh) (33,34).
In both countries, public sector staff salaries data were used to value staff time. The key source of prices for consumables and equipment in Tanzania were the Tanzanian Government’s Medical Supplies Department price lists. Where shipping costs were excluded from prices, we included a 17.4% uplift to account for transportation and insurance as recommended by the MSD. In Kenya, sources included the Kenya drug index catalogue and a 2018 survey of 20 healthcare facilities (35). Where prices were not available locally, we obtained costs from the UNICEF supply procurement list, South African medical supplies price list, experts in critical care in sub-Saharan Africa and, finally, internet searches. Hospital hotel costs were based on daily charge rates for both countries.
The PATH oxygen and costing tool provides a means of estimating the cost per litre per minute of oxygen under different scenarios for different settings (https://www.path.org/resources/quantification-and-costing-tools/). To generate a cost per litre of oxygen using the tool, we were required to provide data on hospital characteristics - including number and type of beds and bed occupancy. We used a scenario for a typical district hospital in Tanzania based on hospital facility surveys (15,36). The PATH costs include transportation and logistics for the oxygen supply as well as back up supply and the power costs and captures both capital and recurrent costs. We complemented this with local prices collected in 2021 (the price for a cylinder refill) (see Supplementary material 2).
Generating unit costs and scenario analysis
A cost per patient day was derived for a reference scenario based on the resource use per patient day for each category of patient for EECC and ACC. A cost per patient was then generated by multiplying this by the average length of stay for different patient categories obtained from the literature (37). For the reference cost scenario, the costs are defined as the costs of EECC resources that need to be in place, without which EECC could not be provided.
Ranges for the cost per patient day were developed based on different scenarios that address uncertainties in the key assumptions for oxygen and staffing. In the case of oxygen, the cost of oxygen and oxygen supplies were increased and decreased by 25%, to capture the fluctuation in prices during the pandemic. In the case of staffing, for a low cost estimate we identified the lowest cost staff that could carry out the tasks from the staff list staff salary costs; for the high cost estimate staff salary costs used were at the highest grade for nurses and a consultant level salary used for the doctor. For ACC, we further varied pharmaceutical costs by increasing and decreasing their total cost per day by 25%.
{kind=link}