IE is a fatal disease with diversity of clinical manifestations and risk factors, continuing to be associated with high mortality despite of novel diagnostic and therapeutic strategies[1]. The demographics, predisposing factors, clinical features, and microbiological spectrum of IE have evolved in recent decades. Relative studies remain scarce in China, and are usually of small sample. Our study was aimed to better understand the regional characteristics and the changing profile of IE over 18 years in our hospital, and to evaluate independent factors that influence the outcome of IE. To our knowledge, this is the largest study on IE performed in our region over 18 years.
Clinical features
The proportion of IVDUs declined by half in later-period group(12.0% vs 25.8%, OR = 0.394, CI: 0.214-0.727) as the Chinese government had been stepping up efforts to crack down drug cartels[12], which might serve as the most important reason for changes of profile of IE for 18 years.
Firstly, patients with IE in the later-period group became older than those from the early-period group (44.9 ± 15.4 vs 36.5 ± 15.2, P<0.001), which was roughly similar to that reported in neighboring regions [9, 13, 14], but far younger than those in developed countries [15-17]. The upward tendency of onset age was probably related to the downward trend of intravenous drugs abusing. Compared with middle-aged and elderly people, young adults are more likely to be exposed to drugs[18, 19]. In addition, the decrease of patients with rheumatic heart disease (from 22.7% to 17.6%) and the increase with degenerative heart disease (from 4.1% to 9.3%), may lead to an increase in patients’ age.
Secondly, the positive rate of Staphylococcus aureus decreased strikingly in the later-period group (20.0% vs 41.3%, OR = 0.355, CI: 0.172-0.732), while the echocardiography results showed a lower proportion of tricuspid valve vegetations in the later-period group, which is linked to the significantly lower proportion of IVDU since it is generally known that IVDU-related IE is more likely to involve Staphylococcus aureus and infection of the tricuspid valve[18, 20]. By comparison, the increase of other gram-positive cocci might be attributed to the relatively uprising of other predisposing factors besides IVDU.
Thirdly, IE patients of the later-period group developed less ischemic stroke (27.3% vs 10.3%, OR = 3.269, CI: 1.592-6.714). Previous studies reported that Staphylococcus aureus infection and vegetations on the mitral valve were risk factors for ischemic stroke[21, 22], but among the patients in this study, the later-period group showed a lower percentage of Staphylococcus aureus infection and a nonsignificant rise in patients with mitral vegetations (34.7% vs 30.9%). We speculate that an older age at onset and a higher proportion of diabetics (10.6% vs 5.2%) may play a more important role in triggering ischemic stroke.
Besides, the decrease of patients with pulmonary embolism (1.9% vs 7.2%, OR = 0.243, CI: 0.069-0.849) in the later-period group could be explained by less numerous right-sided IE. Also, the lower occurrence of renal insufficiency (6.0% vs 15.5 %, OR = 0.350, CI: 0.160-0.768) might be benefitting from the reduction in Staphylococcus aureus infection and the downward trend in cardiac insufficiency (56.5% vs 61.9%) in recent years[23].
Above all, the IVDU played an important role in the changing profile of IE. Beyond the IVDU-related IE, there were still some other points below worth mentioning.
The negative echocardiography results (absence of vegetations) were seen to increase significantly in the later-period group (15.3% vs 6.2%, OR = 2.735, CI: 1.106-6.764). The most frequent explanations for a negative echocardiogram are very small vegetations, non-oscillating and/or atypically located vegetations, or severe, pre-existing lesions from rheumatic heart disease or degenerative heart disease in heart valves[24]. IE Patients in the later-period group had a higher proportion of degenerative valvular heart disease (9.3% vs 4.1%), which manifested as high-density calcification on echocardiograms and was hard to distinguish from vegetations. Also, the overuse of antibiotics may shrink the vegetations, making them difficult to identify by echocardiography.
Splenomegaly was more frequently found in the later-period group (26.4% vs 15.5%, OR = 1.960, CI: 1.046-3.673). This phenomenon had not previously been seen in previous reports, perhaps owing to the development of improvements in imaging technology.
Up to 41.8% of patients were blood-culture negative in our study, which was similar to other region of China(from 31.4% to 51%)[9, 14, 25], far higher than that reported in western countries [5, 15]. Blood culture-negative infective endocarditis is associated with inappropriate antibiotic treatment, faulty culture techniques, atypical pathogens that are difficult to culture or identify[26]. Among these factors, the misuse and overuse of antibiotics remained a problem, especially for patients with long-term fever. The majority (93.1%) of the BCNE patients in our study received empiric antibiotic treatment prior to etiological examination. Atypical pathogens can be identified by serological analysis and polymerase chain reaction (PCR) assays of blood and pathological specimens[27], which is difficult to realize in clinical practice due to economic and subjective factors. With the development of improved microbial culture techniques, increased medical expertise, and more accurate specifications for the diagnostic and treatment processes, the negative blood-culture rate achieved a remarkable decline in the later-period group (37.0% vs 52.6%, OR = 1.890, CI: 1.159-3.077); still, there is room for improvement and research efforts need to be continued.
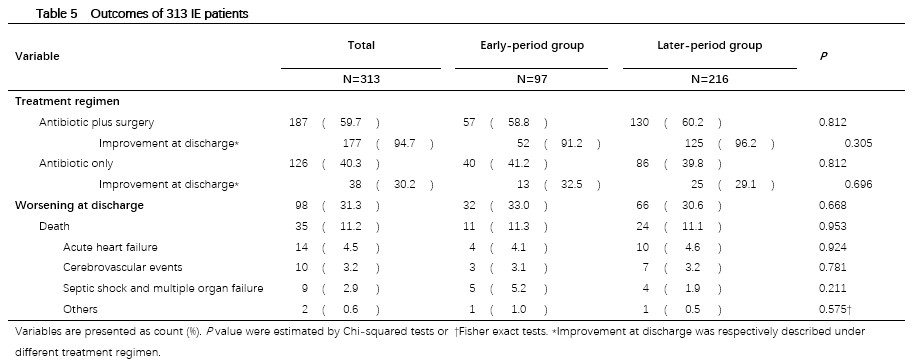
A systematic review of 21 regional literatures in the world revealed that the average fatality rate of IE is 21.1% ± 10.4%[2]. The in-hospital mortality of our study was 11.2%, nearly approaching to the lower limit and quite similar to another research conducted in East China (10.9%). Moreover, it is noteworthy that even with the novel diagnostic and therapeutic strategies available now, the in-hospital mortality did not strikingly differ between the two groups, which means minimizing the in-hospital mortality of IE is still a long-term undertaking.
Risk factors for in-hospital mortality
To explore the independent risk factors for in-hospital mortality, we performed a backward stepwise logistic regression analysis model. The results indicated that health care-related endocarditis[6, 28], prosthetic valve endocarditis[6, 29], intravenous drug users, hemorrhagic stroke, congestive heart failure[14, 30-32], renal insufficiency[30], left cardiac valve vegetations, fungal endocarditis, surgical treatment[6, 32-34] were the independent determinants of in-hospital mortality. Many of them are consistent with conclusions of previous research. But some factors such as age, sex, embolism, although it showed a high influence on in-hospital mortality in univariate analysis, was finally ruled out from multivariate analysis model. It was clearly different from results of previous studies[14, 28, 35]. Perhaps multifarious confounding factors contributed to their analysis results.
Early surgery during antibiotic therapy is a protective factor for prognosis of IE in our study. Mortality of patients who underwent surgery was one sixth of that of patients who did not have the surgery(OR=0.155, CI: 0.054-0.450). In our study, up to 59.7% of our patients underwent valve surgery during the initial hospitalization, which is relative high compared to results observed in other countries[6, 31]. We believe that good standard of care in our hospital, and relatively younger age were a major reason for patients to make aggressive decision of surgical treatment. And we speculated that the relatively lower in-hospital mortality compared to foreign countries, may be mainly contributed by higher rate of surgical treatment and younger age of onset.
It seems that the independent link of intravenous drug users, hemorrhagic stroke, left-sided endocarditis and fungal endocarditis to in-hospital mortality has not yet been pointed out before. The mortality of IVDU-related IE had been reported to be lower than that in none-IVDU-related IE in some studies[36], which was poles apart from our conclusion. Hemorrhagic stroke itself is exactly a highly lethal disease. Left-sided endocarditis was described as independent risk factor for mortality of IVDU-related IE, but not of IE[37]. The fungal endocarditis in our study was of extremely small sample (only 6 of 313) so its veracity of statistical significance deserve suspicion. Consequently, further studies are essential for validation of our conclusions.
limitation
This study focused on a single-center in a general teaching hospital without long-term follow-up. Most patients came from south China, thus findings in this study may not be applicable to all populations. Besides, referral bias should be taken into consideration when describing the clinical spectrum and outcome of IE, as patients with more complications such as stroke, heart failure and new valvular regurgitation and surgery indications, who are more likely to be gravely ill patients, are more likely to choose a tertiary hospital[38]. So our conclusions may not apply to small hospital. However, our observations reflected a dynamic change of IE in our center over a period of eighteen consecutive years with a relatively large sample size, while relative study remains scarce in China. The geographic variations observed in our study will be of important value to profile the clinical feature of China and offer the reference for clinical decisions in our region.
{kind=link}