In this study HBoV was detected in 8.1% of the 333 children recruited. The detection rate observed in this study is higher than 6.8% reported by Moreno et al. in Argentina, 7.2% reported by Tran et al. in Vietnam and much higher than 1.2% reported by Niang et al. in Senegal but lower than 16.8% reported by Symekher et al. among Kenyan children (7,11–13). This difference could be as a result of sampling strategy, severity of illness in the children recruited and different climates. The months of January (41%) and December (30%) recorded the highest number of HBoV infections among the children recruited in the study (Table 2), and this is similar to the finds of Goktas et al. (14) which reveals that HBoV infection activity has a peak period in the months of December to January, which are cold seasonal. This seasonal character could be a result of the cold temperature observed in these months of the year as supported by the findings of Erling et al. (15). Although not significant, females (59.3%) were found to have a higher prevalence of HBoV in this study (Table 3). This is similar to what was previously reported in India by P. Bharaj, et al. and in Saudi-Arabia by Abdel-Moneim, et al., but different from reports by Symekher et al. among Kenyan children and Salmon-Mulanovich et al. among children in South America (13,16–18). Children of age group >1 – 2 years had the highest detection rate and showed symptoms of highest severity (Table 3). This is similar to the findings of (9). Among the symptoms observed in children with HBoV in this study, cough (100%) and catarrh (100%) had the highest frequency, whereas vomiting (11%) tonsillitis (3.7%), and diarrhea (3.7%) were the least observed symptoms (Table 4). The symptoms observed in children positive for HBoV infection in this study, are similar to the reports of Hengst et al., Korner et al., Akca et al. and Moesker et al. (2,6,19,20). This suggests that laboratory screening for HBoV should be included in the management of in the children ≤ 5 years old presenting with cough, catarrh and other respiratory tract symptoms in Nigeria.
Of the 27 HBoV isolate detected in this study, 23 were successfully sequenced. The phylogram generated from the nucleotide sequence of the 23 HBoV isolates in this study and that of HBoV reference strains showed all the isolates clustering with the reference strain of HBoV1 (Figure 1 & 2). This is similar to the findings of Nokso-Koivisto et al., Abdel-Moneim et al. and Principi et al., where they reported HBoV-1 as the genotypes mostly found to be associated with respiratory distress in children (17,21,22).
The phylogenetic analysis revealed that six of the 23 isolates in this study have a very high level of similarity with ST1 and ST2 which are the WHO references strains for HBoV-1 genotype (3) while the remaining 17 isolates showed lower similarity to the reference strains. The six isolates that clustered closely to the references strains for HBoV-1 (Figure 1 & 2) were gotten from children that exhibited symptoms of high severity (Table 4 & 5). This is similar to the findings of Kenmoe et al. and Pogka et al., whose study indicated that HBoV-1 isolates that aligns with the HBoV-1 reference strains are often gotten from children showing symptoms of severe acute respiratory tract infections (23,24). This could be because HBoV -1 reference strains were isolated from children with severe acute respiratory tract illness by Allander et al. (3). The remaining 17 isolates that showed a higher divergence to the reference strains where obtained from children who exhibited less severe symptoms of respiratory tract illness (Table 4).
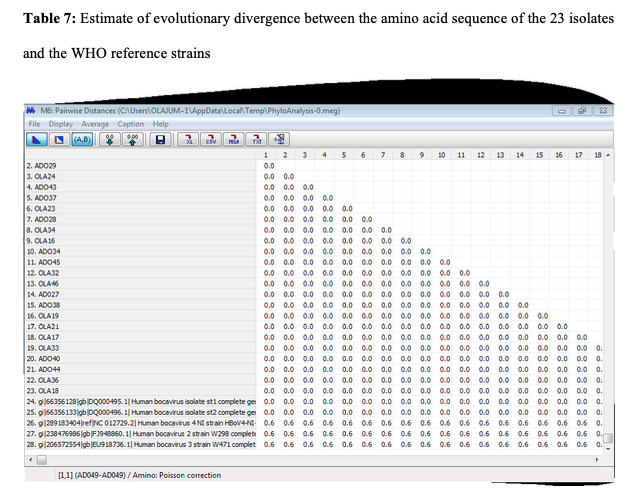
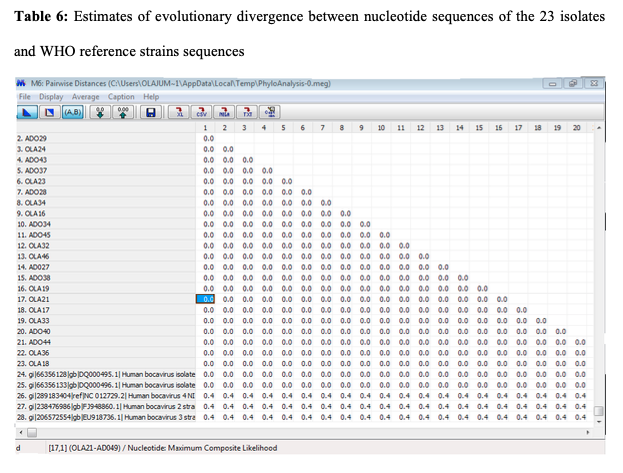
There was low level of diversity in the nucleotide and amino acid differences within the HBoV-1 isolates of this study (that is; an overall mean distance of 0.0 within the isolates and 0.01 when aligned with the WHO reference strain sequences) (Table 6 & 7). This shows the high level of genetic homogeneity exhibited by the HBoV1 isolates of this study, and this supports the findings of Allander et al., Arthur et al., Cheng et al. and Ghietto et al. (3,4,25,26).
When comparing the isolates obtained in this study to other isolates in the Gen Bank it was observed that majority of the isolates were closely related to those from Pakistan. This finding supports those of Kantola et al. and Salmón‐Mulanovich et al., which suggests that there is frequent importation of foreign strains of HBoV-1 genotype, and thereby indicates tourism might plays an important role in the transmission of the virus (18,27).
Finally, the 8.1% prevalence of HBoV1 that was found in this study showed that this virus strain is involved in childhood respiratory tract illnesses in Ibadan, and is therefore of public health importance in Nigeria.
{kind=link}
{kind=link}