Study design
The study was approved by the governmental animal protection committee and the institutional review board for the care of animal subjects. All protocols were approved by the Intervention Technical Center Animal Welfare Committee (IVT-20-66) and experiments were conducted in accordance with the Animal Experiment Welfare Regulations.
Animal model and experimental protocol
As an atherosclerotic model, 4 Watanabe hereditary atherosclerotic (WHHL) rabbits (age: 10 months, mean body weight: 3.2 kg) were used. As a control model, 2 New Zealand white (NZW) rabbits (age: 10 months, mean body weight: 3.9 kg) were used. CMEADM-U at 0.5 mmol Fe/kg was administered 72 hours before CT imaging. The rabbits inhaled isoflurane through a mask and CT was performed under deep anesthesia. Subsequently, after confirming systemic collapse and analgesia under anesthesia control with isoflurane, an axillary incision was made and all animals were exsanguinated through the axillary artery. They were regarded as being euthanized by confirming an SpO2 reaching zero on a bedside monitor and dilation of the pupils. Subsequently, the aorta was collected and fixed in paraformaldehyde. Paraffin blocks were prepared, and hematoxylin & eosin (HE) staining and Berlin blue staining (BB) were conducted using 3-µm-thick axial sections. Furthermore, specimens for immunostaining of macrophages (Macrophage clone RAM11: RAM11) were prepared using 4-µm-thick sections. The association with CMEADM-U accumulation was evaluated. Six sections per animal (total: 24 sections) from the WHHL rabbits and 3 (total: 6 sections) from the NZW rabbits were prepared. For alignment between CT images and pathological slices, the upper margin of the aortic arch and abdominal aorta-common iliac artery bifurcation were used as landmark.
CT protocol and CT analysis
All rabbits were scanned using Aquilion One PRISM Edition (Canon Medical Systems Corporation, Otawara, Japan). This system facilitates rapid kVp switching-type dual-energy scans (135 kVp and 80 kVp). The following imaging conditions were adopted: tube voltage, 135 and 80 kVp; tubal current, 100 and 570 mA; slice thickness, 0.5 mm; tube rotation speed, 0.5 s; rearrangement FOV, 240 mm; and matrix, 512 x 512. For image analysis, Vitrea workstation (Canon Medical Systems Corporation, Otawara, Japan) was used, and a DE-analyzing application, spectral analysis, were adopted. On VMI, image contrasts can be regulated by changing the effective energy. In this study, 35 keV, at which the highest contrast can be obtained, was used. Furthermore, images at 70 keV corresponding to 120 kVp, which is primarily used in clinical practice, were rearranged and compared. In addition, USPIO imaging at different concentrations was conducted, and an iron-based map with the 3-material-decomposition method was prepared by measuring the CT value for each concentration at 85 and 65 keV. For image measurement, the region of interest (ROI) for the vascular wall on each image was established. The CT value (Hounsfiedl unit; HU) was measured from VMI findings and the iron-based map value was from an iron-based map.
Histopathological examination
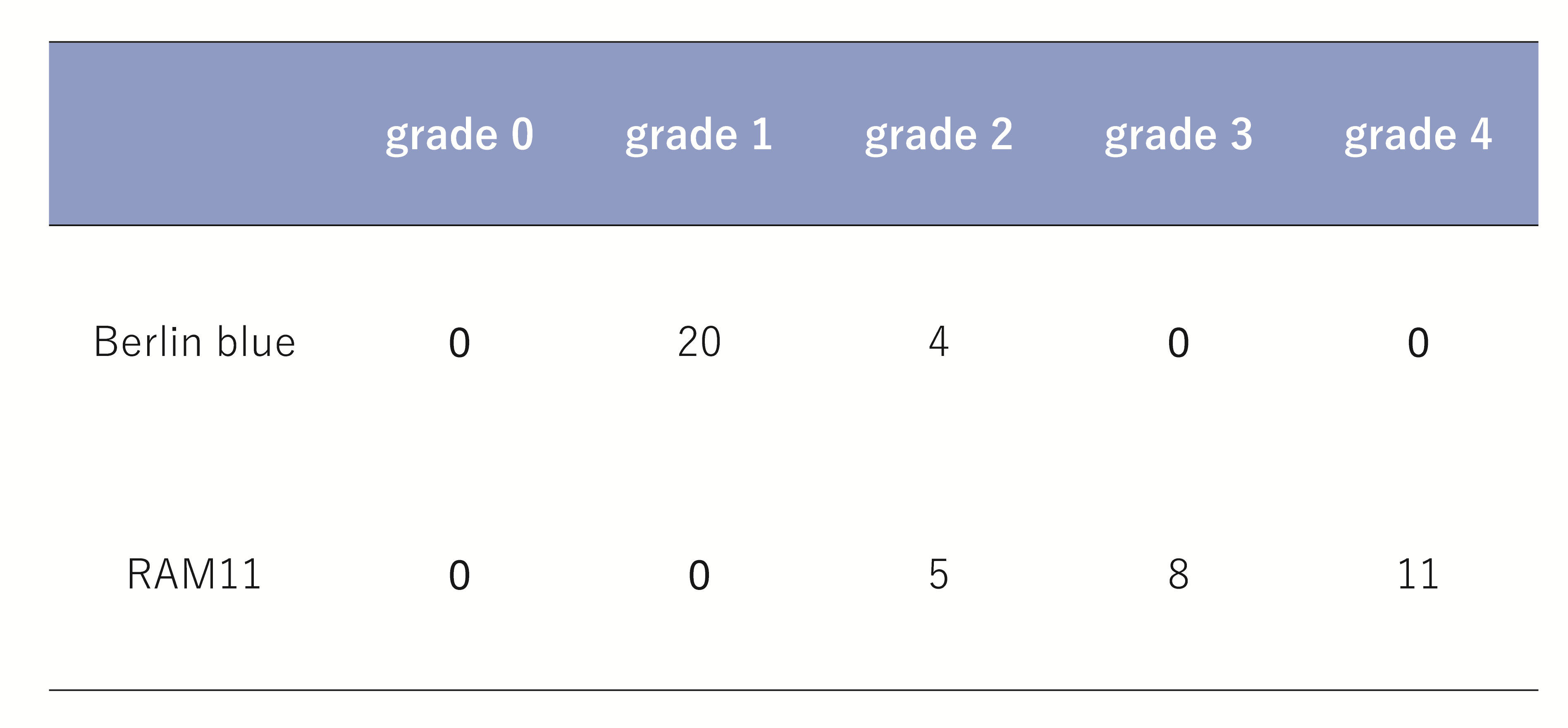
In the WHHL sections, the grade of accumulation on Berlin blue staining and RAM11 immunostaining was evaluated in 5 grades (grade 0: no accumulation, grade 1: ≤1/4 of the inner circumference of the aorta, grade 2: 1/4 to 2/4 of the inner circumference of the aorta, grade 3: 2/4 to 3/4 of the inner circumference of the aorta, and grade 4: entire inner circumference of the aorta) using a BHS binocular microscope (Olympus Corporation, Japan). The results were compared with those of DECT. In addition, for quantitative pathological analysis, virtual slides of the specimens (Aperio ImageScope, SVS mode) were prepared and screen shots of 2.0X zoom images were stored in TIFF format. On the TIFF images, the RAM11-positive area (µm2) was measured using ImageJ (National Institute of Health, U.S.A.) and compared with the results of DECT. The image size was 1,284 x 692 pixels.
Statistical analysis
The data are expressed as the mean±standard deviation. To compare significant differences between two groups, the Student’s t-test was used. For comparison among ≥ 3 groups, the analysis of variance (ANOVA) was adopted. For inter-group comparison, the Tukey honestly significant difference test was used. To examine the correlation between the RAM11-positive area obtained on quantitative pathological analysis and DECT, Pearson’s correlation coefficient was used. A p-value of 0.05 was regarded as significant. Statistical analyses were performed using IBM SPSS ver23 software (IBM Institute Inc., U.S.A.).
{kind=link}