This study is the first systemic review and meta-analysis to systemically evaluate the efficacy and safety of SGLT-2 inhibitor in patients with heart failure. In our meta-analysis of randomized clinical studies, SGLT-2 inhibitor could significantly decrease the incidence of hospitalization for heart failure and all cause death in patients with heart failure. Compared with placebo, SGLT-2 inhibitors could significantly decrease risk for SAE, and didn’t increase occurrence of volume depletion.
Most patients with heart failure suffered from a poor quality of life and high incidence of event rates. Despite advances in the drugs and device for the treatment of heart failure, these population still suffer from symptomatic progression and poor quality of life. Many large clinical studies had indicated that SGLT2 inhibitors had significant reduction in the risk of hospitalization for heart failure in patients with diabetes mellitus[5–7, 14]. All the patients included in these trials were with diabetes mellitus, and most of them didn’t suffer from heart failure at baseline. Whether the heart failure patients without diabetes mellitus could also benefit from the treatment with an SGLT2 inhibitor has not been established. Recently, many large clinical trials has been designed and performed to evaluate the efficacy and safety of SGLT2 inhibitor in heart failure patients with or without diabetes mellitus, and some had been finished[10, 15–19]. We performed the meta-analysis firstly based on the results of these large clinical trials.
For the efficacy outcomes, we observed that SGLT2 inhibitor decreased incidence of hospitalization and all cause death for heart failure as compared with placebo in our meta-analysis. Although many exploratory research has been done, the exact mechanism of the efficacy of SGLT2 inhibitor remain unclear[20]. It is confirmed that patients with heart failure could have a net benefit from SGLT2 inhibitor treatment other than glucose lowering. Thus, our results could further demonstrate the findings of many studies on this subject [21–23].
Our study demonstrated an overall safety profile of SGT2 inhibitors comparable to that of placebo, and the incidence of SAE was similar in both groups. For the reason that SGLT2 inhibitor increases the urinary excretion of glucose and sodium by blocking glucose reclamation in the proximal renal tubules and many patients with heart failure used diuretics at baseline, many experts had potential concerns with volume depletion. However, in our meta-analysis of all these trials, no significant increase was observed in SGLT2 inhibitor group, compared with the placebo.
Our study suggests that SGLT2 inhibitor should be considered in patients with heart failure regardless of presence of diabetes mellitus, given that they safely reduce hospitalization for heart failure and all-cause death in these patients. In future, SGLT2 might be the first choice of hypoglycemic drugs for patients with diabetes mellitus, which increased risk of heart failure and renal disease [24, 25]. Ongoing trials in patients with heart failure will clarify the exact mechanism of the salutary effects of SGLT2 in patients with heart failure in future.
Limitations
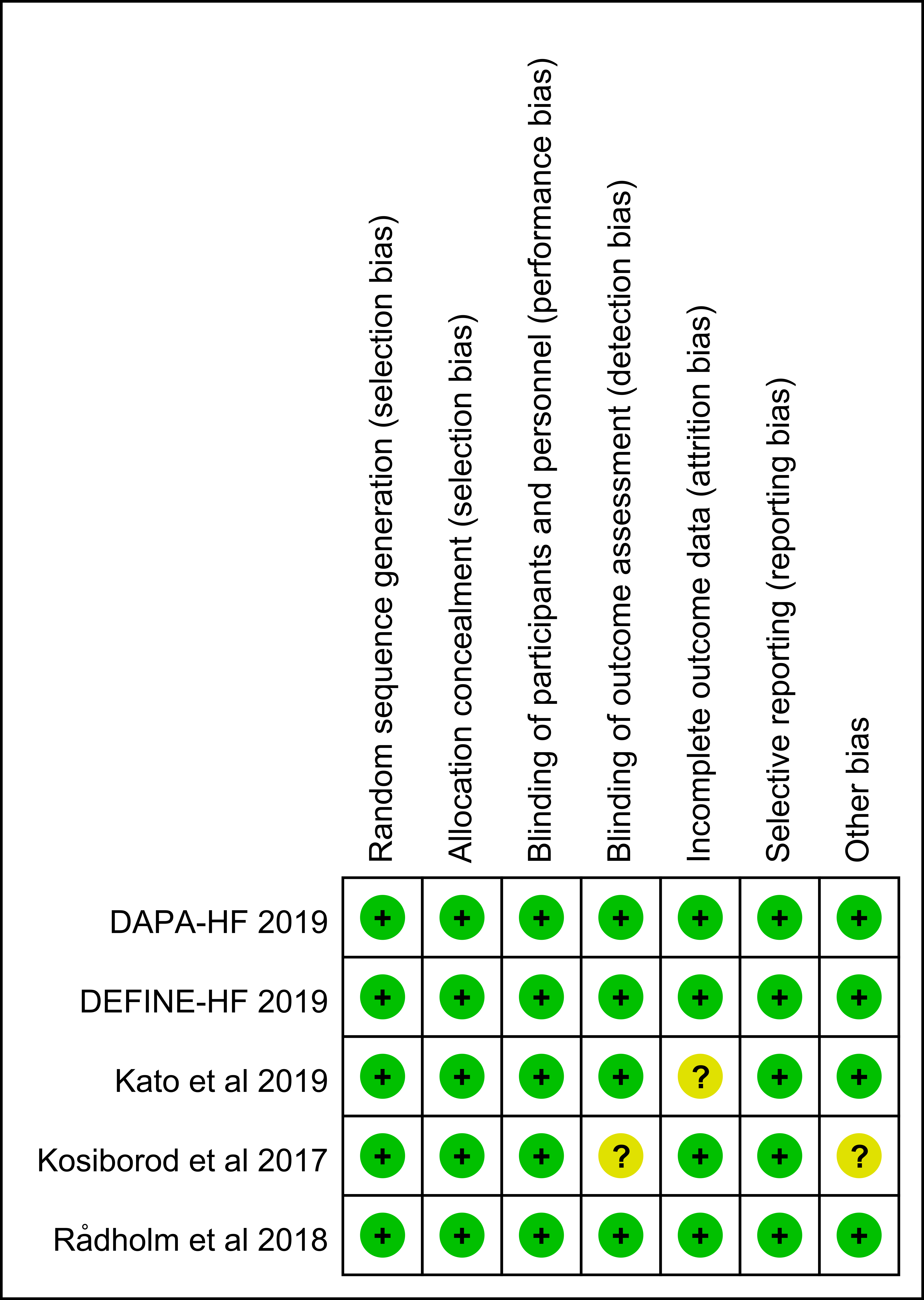
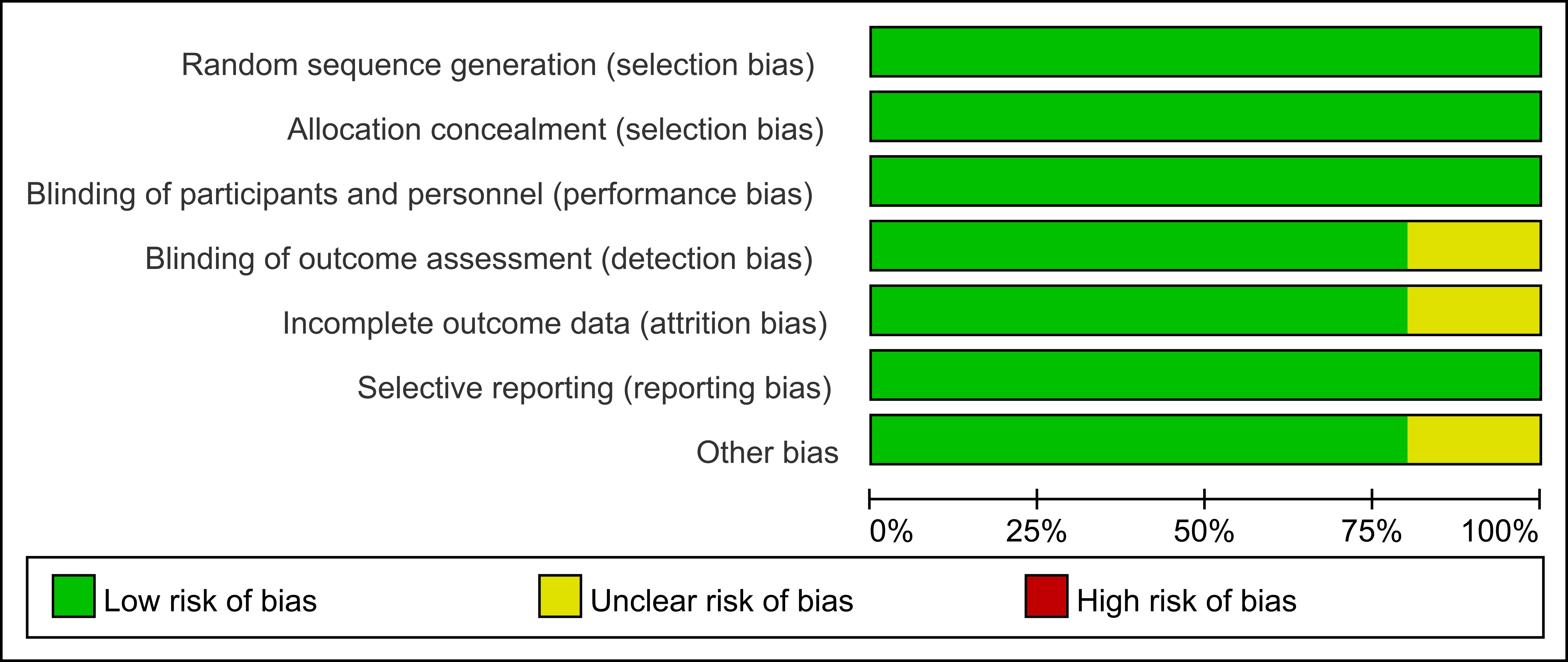
We acknowledge that our study has some limitations. The length of follow-up reported in every study was different from each other, which could be attributable to biases. Besides the type and dose of SGLT2 inhibitor in all trials are not consistent either. We observed a moderate heterogeneity in the results of hospitalization for heart failure and SAE, but both meta regression analysis and sensitive analysis didn’t identify the exact bias. However, we think the final result wouldn’t be greatly affected. More evidence from cohort studies and large clinical trials on the efficacy and safety of SGLT2 inhibitor is thus desirable.
{kind=link}
{kind=link}