Literature selection
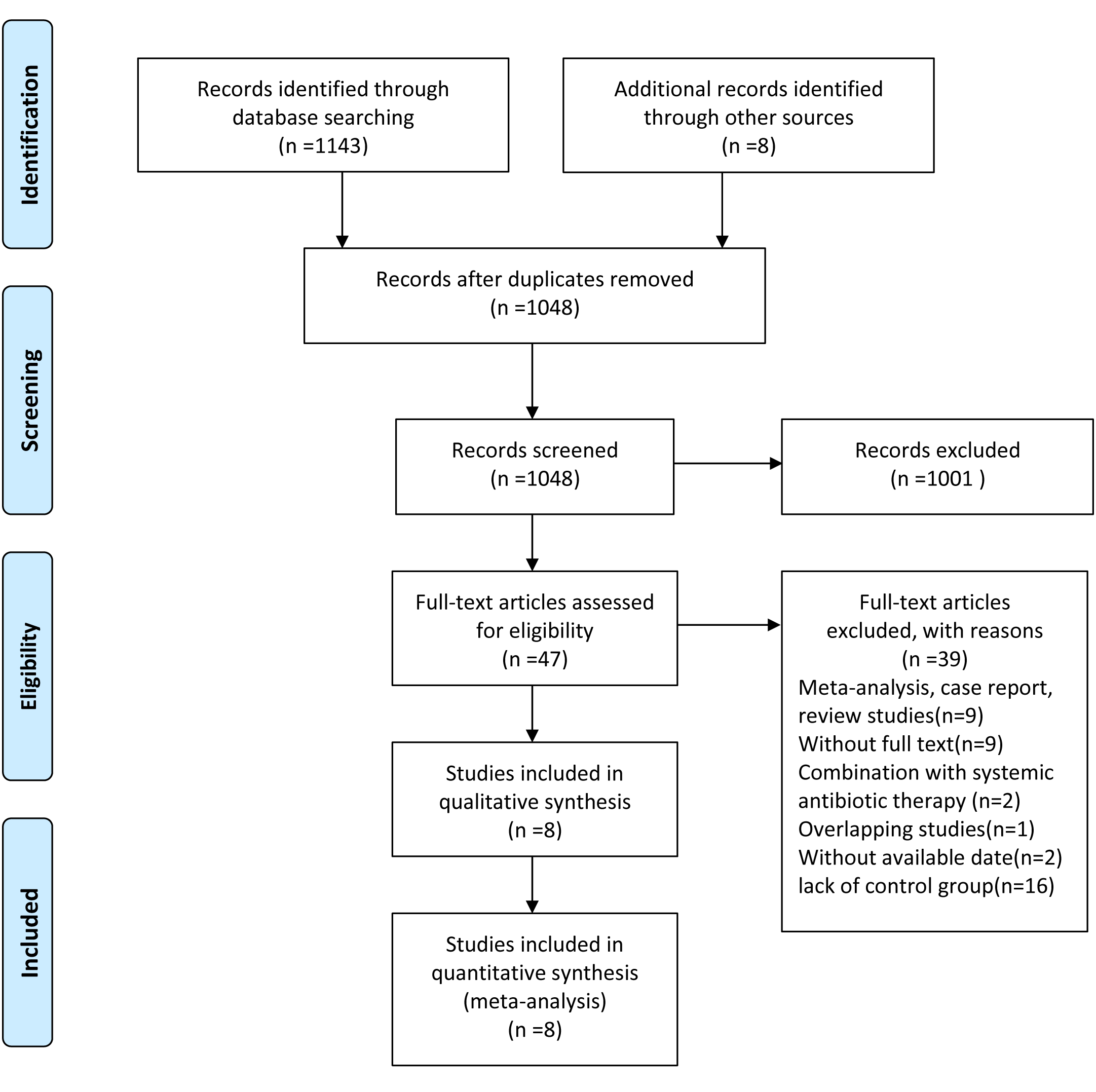
At the beginning, a total of 1,151 records were identified from the electronic and manual search, including 509 in PubMed database, 593 in Embase database, 41 in Cochrane Central Register of Controlled Trials and 8 of manual search. After removal of the duplicates, 1048 publications remained for independent screening, of which 1001 were deemed irrelevant on the basis of their title and abstract and 47 publications were eligible for full-text evaluation. Of these articles, 39 were excluded, mostly because of being meta-analysis, case report, review studies (n=9), without full text (n=9), the combination of systemic antibiotic therapy (n=2), being overlapping study (n=1), without available date (n=2) and the lack of control group (n=16). Finally, 8 RCTs met the eligibility criteria in this meta-analysis. (Supplementary figure S1)
Characteristics of the included studies
As shown in Table 1, main characteristics of the included trials are presented. They were published between 2009 and 2019. There was little variation in the number of participants enrolled in the 8 RCTs (24–36), reaching a total of 247 with mean age ranging between 41.4 and 51.6 years. The studies were carried out in the following countries: Brazil (n=2), Turkey (n=4), China (n=1) and Germany (n=1). The percentages of female participants in the studies were summarized, which ranged between 40.0% and 100%. All studies reported the percentage of female participants, Five of these studies reported a duration of RA from 6 weeks to 14.9 years and three did not provide the duration information. Length of follow-up period varied amongst the 8 included studies, ranging from 1 to 6 months duration. Seven of the studies included outcomes of PI, PD and BOP, four of AL and three of GI.
Risk of bias within studies
The quality of evidence for each outcome was based on six domains: Selection bias, performance bias, detection bias, attrition bias, reporting bias and other bias. Results were presented graphically by study (Fig. 1A) and proportion chart of bias was set across all studies (Fig. 1B). It is noteworthy that only one of the studies was judged to be at high risk of selection bias, which was observed in Roman-torres 2015. Three studies had an unclear risk of bias in blinding of participants and personnel, 4 studies had an unclear risk of bias in blinding of outcome assessment, and 6 studies had an unclear risk of bias in selective reporting. In addition, with regard to allocation concealment, all studies showed unclear risk.
Meta-analysis of clinical indices
The overall effect size showed that the PI value in periodontitis patients with RA changed more significantly compared with periodontitis control patients (MD: 0.42; 95% CI: 0.02, 0.81) (Fig. 2A). Substantial heterogeneity was observed for PI (I2=50.8%, P =0.06). No statistically significant difference was showed between the two groups for the GI (MD: 0.03; 95% CI: -0.03, 0.10) (Fig. 2B). No evidence of heterogeneity was detected for GI (I2=20.8%, P =0.29).
Meta-analysis of clinical parameters
Compared with periodontitis control patients, the changes of the PD (MD: -0.06; 95% CI: -0.18, 0.06), AL (MD: 0.16; 95% CI: -0.03, 0.36) and BOP (MD: 4.15; 95% CI: -0.26, 8.55) were not obvious in periodontitis patients with RA. No heterogeneity was observed for PD (I2=0.0%, P =0.84) and AL (I2=0.6%, P=0.39), and substantial heterogeneity was observed for BOP (I2=50.8%, P =0.06) (Fig. 3A-C).
Sensitivity analysis
Sensitivity analyses were performed in order to assess the potential source of heterogeneity of PI and BOP outcomes. We evaluated the influence of individual dataset on the pooled effect by sequential removal of each eligible study. However, the findings were corroboratively robust and no significant change was detected for all primary outcomes (Fig.4).
Publication bias
Begg's and Egger's test revealed that there was no publication bias for the changes of PI, GI, AL and BOP (P>0.05), but Egger's test manifested that there was publication bias for PD (Egger’s test P=0.04). The trim-and-fill analysis suggested no evidence of significant difference between the adjusted value and the original value of PD changes, but revealed a missing study for BOP changes. At the same time, the adjusted value for BOP changes was also not significantly different from the original value (Table 2).
Subgroup analysis
To determine the potential influence of follow-up time on the clinical efficacy of SRP, we performed analyses separately for different follow-up time points. Compared with periodontitis control patients, the reduction of BOP (MD: 5.93; 95%CI: 0.28, 11.58) was significantly larger in periodontitis patients with RA at the 3rd month after SRP. Similarly, the changes of PI (MD: 0.60; 95% CI: 0.08, 1.13) and AL (MD: 0.36; 95% CI: 0.06, 065) of periodontitis patients with RA were slightly larger at the 6th month than periodontitis control patients (Table 3).
{kind=link}