Diabetes mellitus (DM) represents one of the most common chronic metabolic diseases with increasing prevalence [1]. In type 2 DM, diabetic nephropathy (DN), where proteinuria is the main characteristic, represents one of the most frequent microvascular complication [2]. As early intervention, diagnostic markers are important to detect DN at early stage. It can slow kidney function deterioration and aid in reducing adverse outcomes. Pathologically, kidney hypertrophy is usually shown in DN patients with basement membrane thickening, extracellular matrix proteins deposition, glomerular sclerosis and interstitial fibrosis [2, 3]. Although follow up of DN patients can be done by blood glucose and blood pressure control, progression of renal failure can eventually be seen in many patients [4]. Hence, understanding DN pathophysiology and development of new biomarkers seem to be of high demand for DN early diagnosis.
Cystatin-C, (a low molecular weight protein 13,343 Da), is an endogenous cysteine protease inhibitor that is produced in most tissues. It is found also in all biological fluids [5]. It represents an ideal marker of endogenous glomerular filtration rate. For assessment of renal function, cystatin-c represents a more sensitive parameter than serum creatinine [5].
Several studies reported that cystatin-C is not only an ideal biomarker but also, in critically ill adults, it is associated with recovery prognosis of acute kidney injury [5, 6, 7]. In addition, Taha et al. [8] deduced that, in cadmium nephrotoxicity, cystatin-C is the most applicable biomarker.
Heme oxygenase 1 (HO-1) is known as an inducible enzyme which has different properties e.g., potent antioxidant, anti-inflammatory and anti-apoptotic one. Its activity was shown to occur via breakdown of heme fraction and generate protective products like carbon monoxide (CO) and biliverdin, with subsequent formation of bilirubin and ferritin via iron release from the heme part [9, 10]. Under homeostatic conditions, in the kidney, levels of HO-1 protein remains undetectable, except in the tubules where it is found but in low levels. However, several stress conditions that include oxidative stress, heat shock, hypoxia, heavy metals and toxins) up-regulate the renal transcription HO-1. Under these conditions, heterogenous expression of HO-1 is detected in different renal compartments. In the medulla HO-1 is more highly expressed than the cortex, while in tubules, its expression is found to be very strong (especially proximal tubules). In contrary to glomeruli where minimal or absence in HO-1 expression. In certain pathologies, low glomerular capacity in HO-1 expression is a key cytoprotective mechanism that can explain glomeruli’s particular sensitivity to stressors [11]. At present, in DN, assessment of urinary markers of inflammatory and oxidative processes that are close to tubular damage are recorded as urinary heme oxygenase-1 (uHO-1) [12]. Upregulation of HO-1 in proximal tubule cells was found in response to oxidant stress, so HO-1 seems to be an efficient biomarker of intrarenal activity as well as renal injury [13]. Recent study showed that, in patients with various kidney diseases, HO-1 levels within damaged cells falls away into the renal tubules [14].
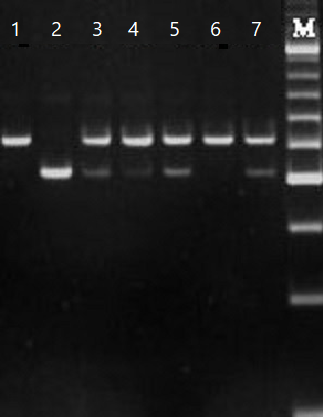
Angiotensin I-converting enzyme (ACE) is a key component of renin–angiotensin system (RAS). Its synthesis was observed in both epithelial and endothelial cells that is located in different organs as lungs, kidneys and blood vessels. Its main function is to catalyze producing vasoactive peptide angiotensin II from angiotensin I (its precursor), in addition to inactivate bradykinin. Besides, angiotensin II has a critical role in maintaining blood pressure, sodium homeostasis and renal hemodynamics. Mahwish et al. [15] reported that ACE gene is located on chromosome 17q23 and spans approximately 21 kb. This gene was shown to include 26 exons as well as 25 introns and encodes a protein containing 1,306 amino acid. Previous records of National Center for Biotechnology Information (NCBI) had shown that ACE gene had more than 160 polymorphisms (mainly single nucleotide polymorphisms (SNP) [16]. Within the circulation, ACE G2350A gene (one of the ACE genes) had demonstrated a significant role in the determination of ACE level [8].
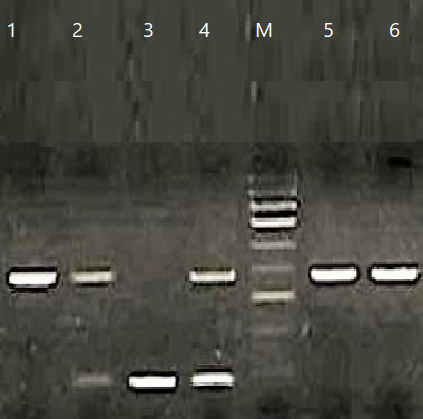
Other polymorphism is the insertion/deletion (I/D) one which represents the most widely studied ACE polymorphism. It is characterized by the presence of a 287 bp Alu repeat sequence (insertion) or absence (deletion) in intron 16. This produces three genotypes (wild I/I homozygous, heterozygous I/D heterozygote, and mutant homozygous D/D) [17, 18]. It was recorded in individuals with DD genotype, higher concentration of ACE in both tissue and plasma ACE in comparison with either ID of II genotypes [19, 20].
Silveira et al. [18] revealed that ACE insertion (I)/deletion (D) polymorphism could cause instability of RAS as well as dysregulation of micro and macrocirculation and electrolytic homeostasis of the kidney. Moreover, it could affect or lead to DN through a direct effect on cellular hypertrophy resulting vascular modulation in the kidney.
Our goal is the assessment of serum cystatin-C clinical significance and urinary HO-1 in the early diagnosis of renal injury (as biomarkers of renal dysfunction) and its association with ACE I/D and A2350G genotypes in T2DM patients.
{kind=link}
{kind=link}