Metabolic syndrome is a complex cluster of conditions which are multifactorial in nature. It is the disorder thought to be caused by an underlying disorder of the energy homeostasis i.e. energy utilization and storage and characterized by co-presence of obesity, insulin resistance, and cardiovascular disorder mainly hypertension (Fawzy et al., 2015). The trends of metabolic syndrome in Asia-Pacific region are scary, nearly 1/5th or more adults are suffering from metabolic syndrome with a secular increase in prevalence (Ranasinghe et al., 2017). International Diabetes Federation (IDF) has estimated that almost 25% of world’s adult population is suffering from metabolic syndrome and they are nearly three times as likely to have a heart attack compared to healthy individuals (Fawzy et al., 2015). IDF has also reported that nearly half (46%, 415 million) of the adult population is living with diabetes, among them almost 90% are having type 2 diabetes (T2DM). It has been found that 40–60% of diabetic individuals develop hypertension as a comorbidity (Jain et al., 2017).
The therapeutic management of metabolic syndrome is a challenge and initially involves diet-life style modification, and when this proven insufficient, then each confounding factor of the metabolic syndrome is treated with medicines (Fawzy et al., 2015;Jain et al., 2017). The first line agent to treat diabetes and particularly in an obese patient is metformin. Metformin (METF) enhances insulin sensitivity, peripheral glucose uptake while suppressing insulin resistance and hepatic glucose production (Fawzy et al., 2015). METF positively affects lipid profile and hemodynamic indices (Setter et al., 2003). METF action is believed to be mediated via activation of AMP-activated protein kinase (AMPK) (Fawzy et al., 2015). Hypertension is another important characteristic of metabolic syndrome and one of the most preferred antihypertensive drug is Telmisartan (TELMI), which belongs to the class of angiotensin receptor blockers (blocks angiotensin II receptor). It is interesting to note that, proliferator activated receptor-γ (PPR-γ) that has a role in carbohydrate lipid metabolism gets modulated by TELMI, and thereby it also helps to control metabolic syndrome (Kurtz, 2005;Fawzy et al., 2015). Telmisartan has the highest binding for PPR-γ among an entire class of antihypertensive agents (Sengupta et al., 2017). Fujimoto et al. have shown that TELMI increases the GLUT4 protein expression and glucose uptake (Fujimoto et al., 2004). Apart from this TELMI also lowers baseline insulin level in metabolic patients (Kurtz, 2005).
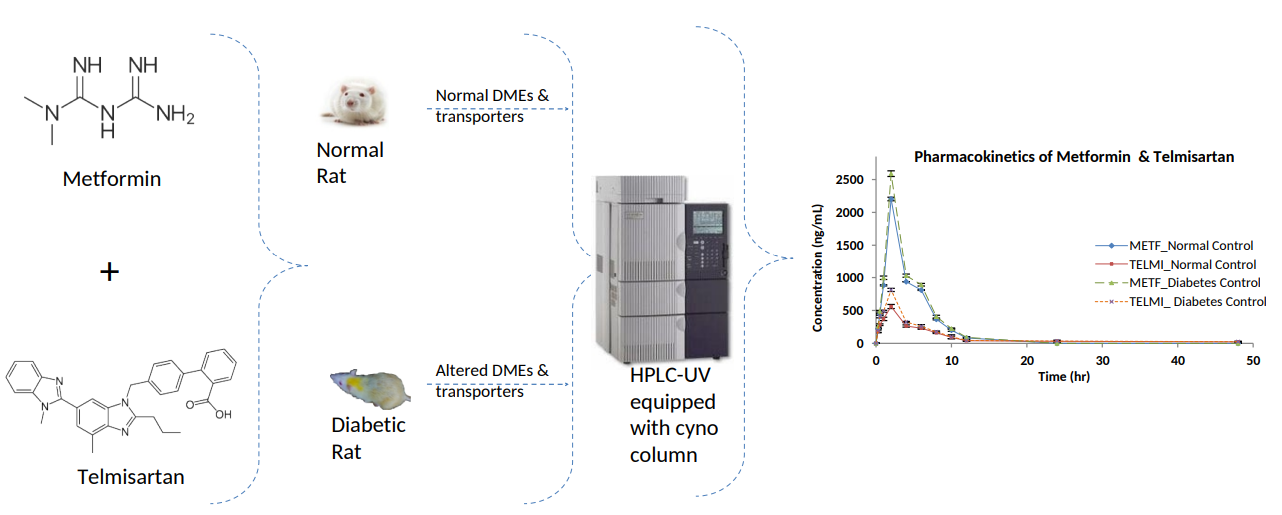
METF a first line of drug which is substrate of PMAT, SERT, MATE1, BCRP, OCT1, OCT2, and OCT3 transporters those are present in the liver, kidney, and intestine(Kimura et al., 2005;Wishart et al., 2007;Graham et al., 2011;Nakamichi et al., 2013;zu Schwabedissen et al., 2014). METF gets metabolized by drug metabolizing enzymes (DMEs) CYP2C11, 2D1, 3A1/2 (Choi et al., 2008;Lee et al., 2008). While TELMI is substrate of OATP1B3, OATP2B1, Pgp, ABCC2, BCRP, and OATPB3 transporters present in liver, intestine and/or kidney. TELMI gets metabolized by UGTs(Kimura et al., 2005;Choi and Lee, 2006;Wishart et al., 2007;Deppe et al., 2010;Graham et al., 2011;Nakamichi et al., 2013;zu Schwabedissen et al., 2014). As diabetes is one of the chronic complex multifactorial diseases, leads to alteration in many DMEs and transporters. For instance the level of CYP1A1, 1A2, 2A1, 3A1, 3A4, 4A1, 4A2, 2B1/2, 2C12, 2E1, FMO, CYP2D6, are increased; while CYP2A2, 3A2, 2C9, 2C11, 2C13, 2C22, 2D2 are decreased (Li et al., 2012;Lavasani et al., 2013). In diabetes the transporters MDR1/P-gp, OAT2, OCT2, MRP2 & 4, NTCP, and BCRP show organ dependent alteration in the expression level (Dostalek et al., 2012;Gandhi and Ghose, 2012). Thereby diabetes holds potential to affects METF and TELMI disposition and their PK-PD profile too. Therefore, it is important to understand the degree of in vivo disease(s)-drug(s) interactions of METH and TELMI in diabetes when administered simultaneously.
Above discussion focuses on the importance and need for rapid, sensitive, economical and reliable chromatographic methodology for the simultaneous determination of the METF and TELMI to understand their PK during the pre-clinical trials and therapeutic drug monitoring. However, there are many methods available for this, but they all are mainly for a single drug. While, recently Fawzy et al. have developed a method for simultaneous estimation of METF and TELMI from human plasma and also check its invivo PK application using UPLC-MS/MS (Fawzy et al., 2015). Indeed, the data provided by UPLC-MS/MS is with a high degree of interpretability than HPLC. It is important to note that such expensive, hyphenated, and highly sophisticated instruments are not available in all the laboratories. Therefore, there is need of the hour to develop a suitable method for simultaneous estimation of METF and TELMI from human/rat plasma for a PK application using HPLC. HPLC provide different types of advantages over UPLC-MS/MS. HPLC is economical, requires less degree of expertise, and easy than UPLC-MS/MS and also able to achieve the same objectives of understanding the PK of the drug under study. Therefore, here we have developed a simple RP-HPLC-UV method for the simultaneous estimation of METF and TELMI from rat plasma for PK application and evaluated the PK in diabetic verses normal rats.
{kind=link}