Many previous studies have examined the TME landscape from the perspective of multiple m6A regulators. This provided an idea for our study. Multiple m5C regulatory factors were included in this study to investigate the effects of m5C modification on tumor growth, tumor immunity and anti-tumor under the interaction of multiple m5C regulatory factors. To clarify the different roles of different m5C modification patterns in TME cell infiltration will be helpful to understand the anti-tumor immune response effect of TME under m5C modification pattern, and to guide more effective immunotherapy strategies.
In this study, three different m5C modification patterns were revealed based on 10 m5C regulators, all of which had significantly different characteristics of tumor microenvironment cell infiltration. M5Ccluster A was summarized as immune-desert type, characterized by immunosuppression and early activation of anti-tumor cytokines; m5Ccluster B was summarized as immune-excluded phenotype, characterized by amount innate immune cell infiltration and stromal activation; m5Ccluster C was summarized as immune-inflammatory and metabolic reprogramming phenotype, characterized as strong humoral immune and acid metabolism activation. The immune-desert and immune-excluded phenotypes can be considered as non-inflammatory tumors, with little or no immune cell infiltration in the TME. The immune-inflammatory phenotype was known as a thermo tumor and was characterized by extensive immune cell infiltrates in the TME[32–35]. Although a large number of immune cells also existed in the immune-excluded phenotype, they only existed in the stroma around the tumor cell nest and failed to break through the tumor matrix to kill tumor cells or inhibit tumor cell proliferation. In some tumors, immune cells may be confined to the stroma of the tumor, or they may be present in the tumor itself, resulting in the appearance of immune cells within the tumor [36, 37]. In fact, tumor active stroma is thought to inhibit immune cells [38]. Therefore, we inferred that the activated matrix inhibits the anti-tumor ability of immune cells.
In our study, m5CcluserA showed little or no infiltration of immune cells, with high expression of Tregs and multiple anti-tumor cytokines. Previous studies have found that Tregs can help suppress immune surveillance in tumors, thereby promoting cancer progression[39]. At the same time, it had also been proved that naive B cells can inhibit the growth of cancer cells by secreting four factors that negatively regulate cell growth, and naive B cells inhibited the growth of cancer cells in the early stage and promoted the growth of cancer cells in the late stage [40]. M5CclusterB showed significant mesenchymal activation, and its mesenchymal score was much higher than that of the other two clusters, including high expression of adhesion factors and ECM receptors, which was considered as T cell inhibition. M5CclusterC showed an extensive immune cell infiltration in TME. These findings substantiated the reliability of our phenotypic classification of m5Ccluster, which may help us understand the m5C modification pattern in bladder cancer.
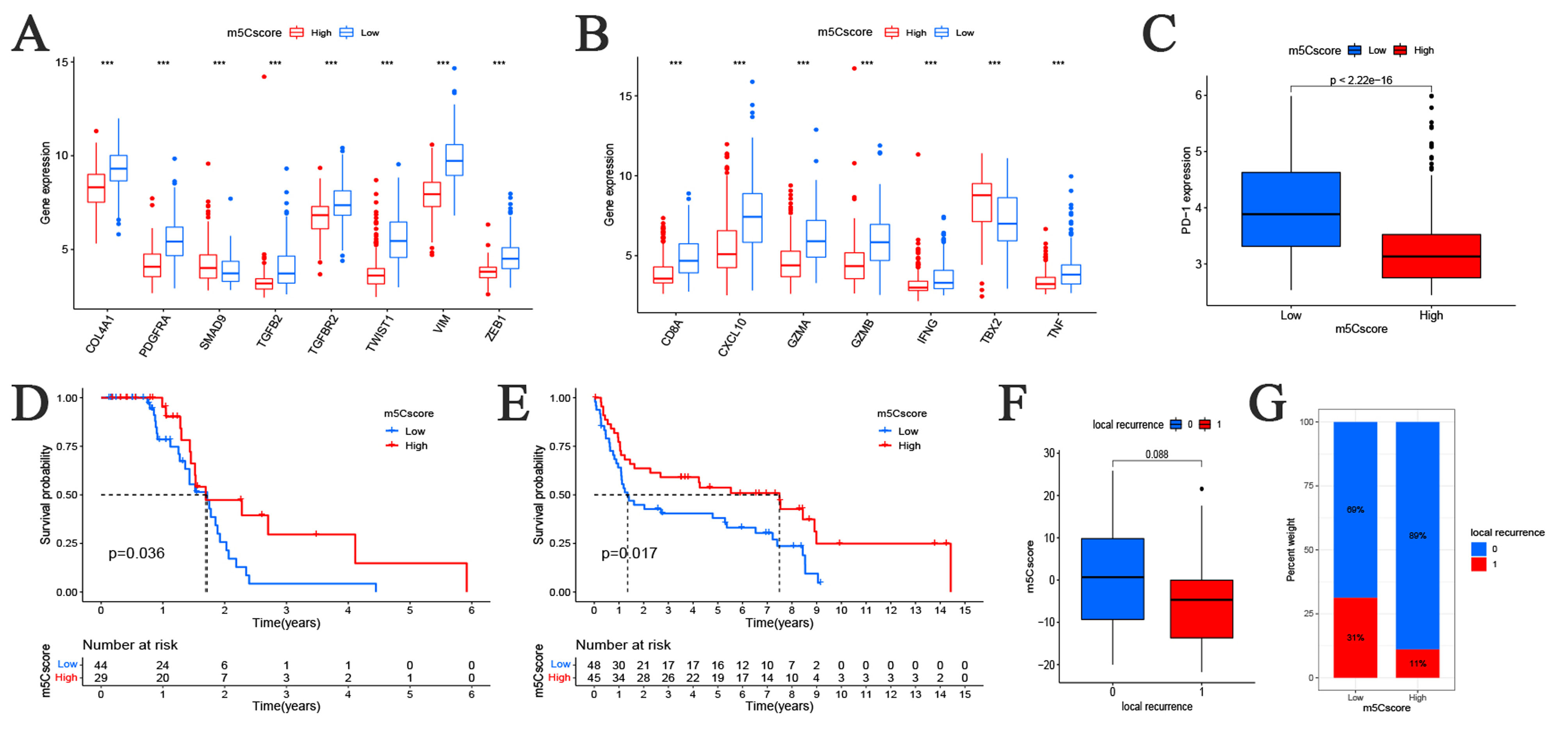
Moreover, mRNA transcriptional differences between different m5C modification patterns further confirmed that m5C was significantly correlated with immune-related biological pathways. These DEGs were considered to be characteristic genes associated with m5C. The prognostic characteristic genes were selected by univariate Cox regression analysis, and then three gene clusters were determined based on prognostic characteristic genes, which were also related to matrix and immune activated pathways. This finding proved that the alteration of m5C is significantly related to the heterogeneity of TME landscape again. Therefore, comprehensive evaluation of the m5C modification pattern would contribute to understanding the characteristics of TME cell infiltration. Considering the individual differences of m5C modification, we needed to quantify the m5C modification pattern of a single tumor. To this end, we constructed a scoring system to assess m5C modification patterns in bladder cancer individuals – m5C score. The m5C modification pattern characterized by immune-desert phenotype showed a higher m5Cscore, while the m5C modification pattern characterized by immune-excluded phenotype exhibited a lower m5Cscore, and higher m5Cscore was associated with a greater survival advantage. Additionally, the immunophenotyping cohort well validated the above results (IMvigor210). These results suggested that m5Cscore could be used as a reliable tool to assess the individual m5C modification patterns comprehensively and to further determine tumor immunophenotypes. Our data also showed a positive correlation between m5Cscore and TMB and the expression of immune checkpoint PD-L1 and PD-1 was also significantly different in the high and low groups of m5Cscore. In our evaluation of clinical traits of patients assessed by m5Cscore, m5Cscore also showed strong predictive ability. M5Cscore can be used to evaluate the survival rate of patients at age, sex and stage of tumor progression. Patients with different clinical traits had significant differences in high and low m5CScore, and there were significant stratifications.
Previous studies showed that matrix activation played a critical role in response and resistance to checkpoint immunotherapy[41, 42]. In addition, activation of Tregs, expression of multiple anti-tumor growth factors, TGF-β and other pathways were associated with activation of EMT and matrix[43, 44]. It had also been proved that the activation of TGF-β and Tregs leads to a decrease in the amount of T cells entering the tumor and a decrease in the killing ability of the tumor[45]. In conclusion, matrix activation had the ability to weaken TME immunity and mediate resistance to immune checkpoint blocking therapy, thus influencing the individualized immunotherapy of bladder cancer. In our study, the methylation pattern of m5C played an important role in the formation of different substrates and the immune TME landscape, suggesting that m5C modification may influence the therapeutic effect of ICB immunotherapy. M5C gene markers include multiple biomarkers such as TMB, PD-L1 expression, neoantigen load, immune TME, Tregs expression and matrix, suggesting more effective immunotherapy prediction strategies. Furthermore, we substantiated the predictive value of m5Cscore in immunotherapy for anti-PD-L1 and anti-PD-1 cohorts. There were significant differences in patients' response to treatment and survival prognosis between high and low m5Cscores.
In conclusion, m5Cscore can comprehensively assesse the methylation modification pattern of m5C and the corresponding characteristics of immune cell infiltration in clinical practice, so as to further evaluate the immunophenotype of tumor. Meanwhile, m5Cscore can evaluate clinicopathological characteristics of patients, including clinical stage, tumor differentiation level, genetic variation, tumor mutation load and neoantigen load, etc. In addition, m5Cscore can be used as an effective independent prognostic biomarker to evaluate the prognosis of patients, and it can also be used to predict the clinical response to anti-PD-L1 /PD-1 immunotherapy. Moreover, our study has provided some novel insights into the mechanisms of TME landscape change and tumor immunotherapy. For example, modifying the mode of modification targeted at m5C regulation and genes associated with the m5C phenotype to further reverse the TME immune cell invasion or stromal invasion, which transforms the "cold tumor" into a "hot tumor". Contribute to the development of new immunotherapy drugs for cancer in the future. Our results provide new ideas for identifying different tumor immune TME phenotypes, improving patients' clinical response to immunotherapy, and promoting personalized treatment of tumors.
{kind=link}