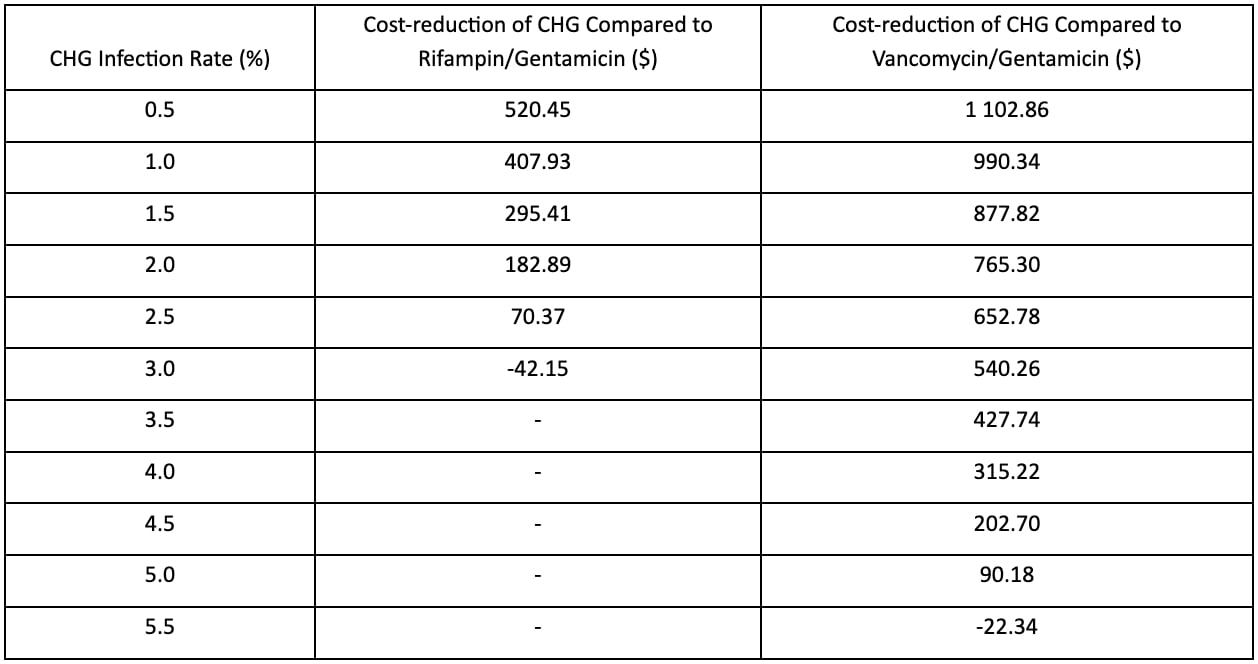
Infections after IPP surgery are frustrating and costly. This study demonstrates a definite target window where CHG irrigant serves as a cost-effective modality for infection prevention. This finding was attributed to a lower incremental complication cost seen when using CHG compared to commonly used irrigation methods like Vancomycin/Gentamicin and Rifampin/Gentamicin, so long as an infection rate of less than 2.8% was observed.
Traditionally, infection rates following IPP placement have a moderate degree of variation based on whether the penile prosthesis is coated or non-coated/hydrophilic and on the compounds impregnated into the penile coating. A previous study displayed infection rates of 2.32% for non-coated prostheses and 0.89% for coated prostheses [2]. Therefore, if CHG demonstrates a similar performance in infection prevention to historically used regimens, it will serve as a cost-effective intervention.
While CHG clinical trials in prosthetic urology are ongoing, it has been employed in other surgical fields. CHG utilization in orthopedic surgery as a washing solution for joint arthroplasty performed very similarly to standard betadine wash, with no significant difference in the rate of wound complications or return trips to the operating room [6]. The field of plastic surgery has also used CHG for breast pocket irrigation prior to implant-based breast reconstruction. In this arena, CHG displayed significantly lower rates of both total complications (22.4% vs. 31.8%, p = 0.006) and infections (6.4% vs. 12.7%, p = 0.006) when compared to a triple-antibiotic solution, although this came at the cost of an increased rate of delayed wound healing (2.9% vs. 0.3%, p = 0.006) [3].
CHG use in urology for IPP placement is likely to be effective. Common bacteria in IPP infection include E. coli, coagulase-negative Staphylococcus spp, S. aureus, P. aeruginosa, K. pneumoniae, Candida, and Group B Streptococcus spp [7, 8]. In lab studies, CHG has shown > 99% efficacy against these common pathogens [9, 10]. If this trend continues into the implementation phase in the operating room, a cost reduction of several hundred dollars may be observed as seen in Table 1. Urologists will need to study if CHG use has any effect on delayed healing rates as observed in plastic surgery.
One of the limitations to this study is the limited nature of the modeling time frame. A 5-year cycle length run for one cycle was configured into the Markov decision tree which excludes any observed differences in outcomes past the 5-year time frame. This investigation was also entirely based on best-case modeling. No IPP clinical trials are completed yet. Another limitation to this study involves not factoring in potentially increased infection rates during salvage operations for penile prosthesis. Previous studies have shown that revision surgeries for mechanical failure, infection/erosion, or patient dissatisfaction have been associated with infection rates ranging from 5.7–10% [11, 12]. The Markov analysis used in this study did not factor in the potential for continued health care costs following initial salvage for infection/mechanical failure. The decision tree treated each salvage procedure as having a 100% success rate. Lastly, this study did not take into consideration quality-adjusted life years during cost-effectiveness analysis. QALYs are a routine measurement in cost-effectiveness analysis as they can serve as a balance between the overall cost-savings in dollars and patient satisfaction/quality of life. Unfortunately, utility values for health states following IPP surgery are limited and dated, and therefore excluded from this study. Future investigation of cost-effectiveness for CHG or any other irrigants will need to have an assessment of QALY, to then balance the weight of direct financial benefit with potentially different patient experiences following IPP placement.
Inflatable penile prosthesis for erectile dysfunction after first-line treatment failure serves as an effective management strategy. However, along with surgical intervention comes the expense of a more invasive intervention that carries a risk for infection. Intracorporeal irrigation using CHG has a lower baseline cost than other standard intraoperative antibiotic regimens and has a potential for equivalent or superior infection prevention, making it an intriguing option for use in IPP surgeries. While the infection rates obtained from other surgical fields when using CHG are promising, clinical studies are underway to investigate this for IPP placement.
{kind=link}