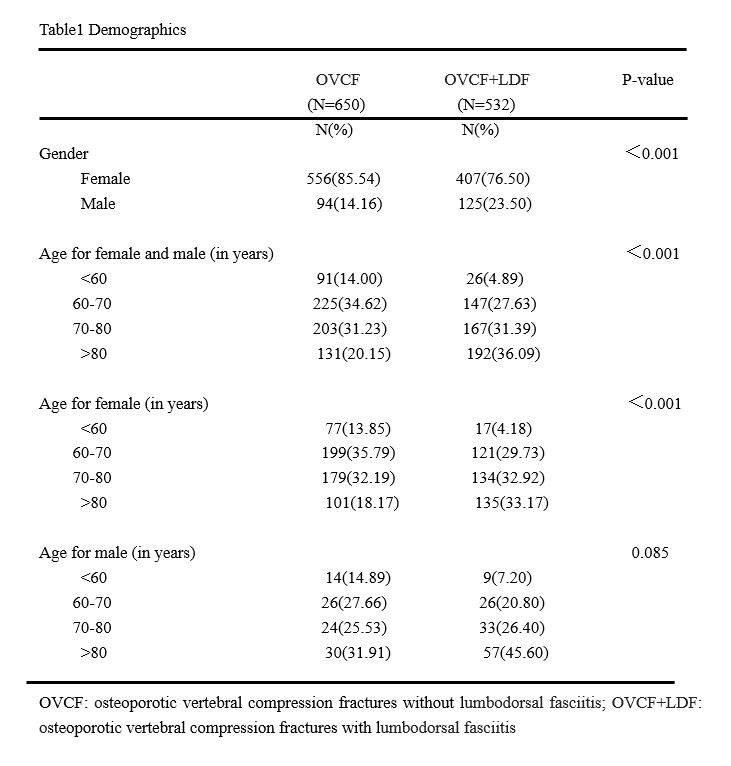
Until recently, concomitant lumbodorsal fascia edema in OVCF has long been underestimated with a less unified diagnosis of posterior fascia oedema[3, 15], thoracolumbar fascia injury[13, 16], and lumbodorsal fascia contusion[14]. The reported incidence also varied significantly from 7% in 268[3] to 50% in 120 OVCF cases[14]. To date, this was the first study specifically investigating its incidence and risk factors in a large study population of 1182 patients. Based on the increasing evidence of sensory innervation in thoracolumbar fascia and inflammation sensitized dorsal horn neurons[6–12], lumbodorsal fasciitis was used here to unify the radiological detection of edema signal along and dorsal to the thoracolumbar fascia. We showed for the first time that concomitant lumbodorsal fasciitis was high as 45% in OVCF without previous spine surgery. As was reported previously patients with thoracolumbar fascia injury were on average older than those without fascia injury[13], an average age of 72.19 yrs old in this study might contribute to the higher global incidence of lumbodorsal fasciitis than in previous reports[3, 15, 16].
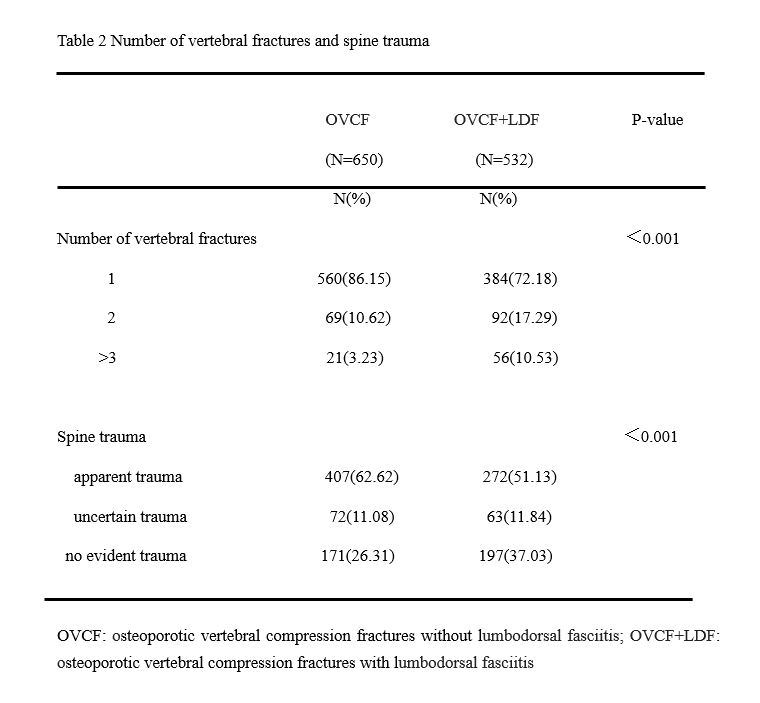
Besides from older age as a risk factor for lumbodorsal fasciitis[13], it remains largely unknown what causes edema in lumbodorsal fascia. Here we showed that increasing age significantly increased lumbodorsal fasciitis in OVCF patients, especially in the females. Besides, males were at higher risk than females to develop edema in lumbodorsal fascia. As paravertebral muscle degeneration is common in aged population[17, 18], the age-related increase of lumbodorsal fasciitis may indicate a degenerative change of multifidus and erector spinae muscle during aging[5], and in males the degeneration is probably accelerated by chronic heavy burdens and lumbar muscle strain[19, 20]. As spine trauma remains the leading cause of vertebral fractures, it is possible the lumbodorsal fasciitis is also caused by the trauma that compressed vertebrae[13]. However, just on the contrary, we found that lumbodorsal fasciitis was significantly increased in the non-traumatic OVCF, suggesting fascia edema might have already occurred prior to or newly developed after vertebral fractures in those with degenerated paravertebral muscle. In support of this notion, lumbodorsal fasciitis was significantly increased in patients with prolonged pre-hospital back pain. Besides, OVCF involving multiple vertebra had higher risk of pre-existing or developing fascia edema, indicating of a reciprocal interaction between paravertebral muscle degeneration and OVCF. Accordingly, we propose a muscle-vertebrae interaction model: lumbodorsal fasciitis tends to occur in aged patients with paravertebral muscle degeneration potentiating non-traumatic and multiple OVCF, the OVCF in return accelerates the degeneration of paravertebral muscle and lumbodorsal fasciitis probably by reducing vertebral height and inducing kyphosis.
Given that lumbodorsal fascia is innervated and could be a potential source of low back pain[6–12], it is intriguing to understand how lumbodorsal fasciitis will effect on the induction and relief of back pain associated with OVCF. Here we showed that patients with lumbodorsal fasciitis more often complained longer duration of back pain before hospitalization, suggesting a possible contribution of the fascia-originated pain to distract patients from the fracture-induced pain. It has been recently revealed that myofascial pain is associated with decreased fascia mobility and increased stiffness that could be induced in thoracolumbar fascia by injury and movement restriction[21–23]. Therefore, conservative therapy like bracing and bed rest might contribute to the higher incidence of lumbodorsal fasciitis in the OVCF with prolonged pre-hospital back pain. Reasons for delayed hospitalization were not investigated in this study, but may presumably include concern of surgical risk or complications in much aged patients with multiple comorbidities[24, 25]. We found that lumbodorsal fasciitis was significantly increased in those with cardio-cerebrovascular comorbidities such as hypertension, coronary heart disease, and cerebral infarction, but not in those with diabetes or chronic pulmonary disease. The close association between cardio-cerebrovascular disease and lumbodorsal fasciitis may indicate a shared pathophysiological basis, or a possibility of antiplatelet and antithrombotic medication in promoting fascia edema, which requires further prospective studies with long-term follow-up.
This study was limited in its retrospective nature and included OVCF patients from a single center. Secondly, VAS score of back pain was not collected and compared between the group with and without lumbodorsal fasciitis. Based on the high incidence (45%) of fascia edema in OVCF and significant pain relief after vertebroplasty, lumbodorsal fasciitis was expected to cause mild and non-specific pain in the lower back[20]. Thirdly, other related factors such as radiographic parameters of regional or global kyphosis[3, 15], body mass index (BMI)[17], and quantified paravertebral muscle degeneration[17–19] were not evaluated to fully understand the promoter of fascia edema. Further prospective studies with stratified participants and long-term follow-up are warranted for a better understanding of the risk factors and pathogenesis of lumbodorsal fasciitis.
{kind=link}
{kind=link}