The sample included 86 patients diagnosed with MDD, 22 patients diagnosed with BP-I and 37 patients diagnosed with BP-II. There were also 281 putatively healthy controls (Table 1).
There were no differences by gender or maximum education level among participants; controls were marginally younger than the patients (partial eta-squared=0.020).
Clinical data were available for patients only. There was no relevant difference in the age of onset of the psychopathology among groups. A family history of depression was observed more often in patients diagnosed with BD-II, while a family history of bipolar disorder was observed in just 5% of patients diagnosed with MDD and in about 25% of those diagnosed with BD (Table 1 for details).
Patients diagnosed with BD-I were more likely to have attempted suicide and have been more often admitted to a psychiatric service than patients with MDD or BD-II. A prescription of an antidepressant was received by most patients, with no differences by diagnosis. A second-generation antipsychotic was prescribed in about 10% of cases, again with no difference by diagnosis. Lithium was rarely prescribed and only in patients diagnosed with BD-I.
Overall, 86 patients with MDD, 58 patients with BD (either BD-I or BD-II), and 265 controls completed the MDQ; while the HCL-32 was completed by 64 patients with MDD, 32 with BD, and 225 controls.
3.1. Floor or ceiling effects
There were no floor effects for the MDQ: 25 controls (8.9%) and just 1 with MDD (1%) scored zero on the MDQ (÷2=11.85; df=2; p=0.003). However, a modest ceiling effect was observed for the MDQ: 4 controls (1.4%) and 11 patients with BD (17.7%) scored 13 on the MDQ (÷2=44.38; df=2; p<0.0001).
There were no floor and ceiling effects for the HCL-32. Overall, in the sample 7 patients scored zero on the HCL-32: 5 controls, 2 with MDD, none with BD (÷2=1.28; df=2; p=0.52). No participants scored 32 on the HCL-32.
3.2. Reliability of the questionnaires
Cronbach’s alpha for MDQ was 0.79 (95%CI: 0.76 – 0.83) in controls; 0.78 (0.75 – 0.82) in patients with MDD; and 0.71 (0.60 – 0.81) in patients diagnosed with BD. Cronbach’s alpha for HCL-32 was, respectively, 0.85 (0.82 – 0.87) in controls, 0.80 (0.74 – 0.85) in MDD, and 0.76 (0.68 – 0.85) in BD.
3.3. Confirmatory factor analysis of the factor structure of the MDQ and the HCL-32
For both the MDQ and the HCL-32, the bifactor implementation of the two-factor model had the best fit according to the predefined parameters (Table 2).
For the bifactor model of the MDQ, H=0.79, ECV=0.54, PUC=0.60, and ùH=0.64.
For the bifactor model of the HCL-32, H=0.80, ECV=0.33, PUC=0.48, and ùH=0.37.
Thus, for both the MDQ and the HCL-32 there is some indication in favor of a single, reproducible latent component. However, the multidimensionality in the data might influence the results that can be derived from a global summary score.
3.4. Discriminant capacity of the MDQ and the HCL-32
Patients diagnosed with BD scored higher than patients diagnosed with MDD and controls on both the MDQ and the HCL-32 (Table 3).
According to the epsilon-squared effect size (Tomczak and Tomczak, 2014), about 20% of the variance in the sample was attributable to the differences in MDQ by groups, and 10% was attributable to the differences in HCL-32 by groups.
3.5. ROC analysis
The MDQ and the HCL-32 were able to distinguish patients diagnosed with BD from putatively healthy controls, with better AUC in MDQ (82.7; 95%CI: 75.3 – 90.2) than in HCL-32 (73.4; 63.9 – 83.0) (Figure 1).
The MDQ (AUC: 88.9; 81.4 – 96.3) and the HCL-32 (AUC: 83.3; 74.5 – 92.1) were equally able to distinguish patients diagnosed with BD from patients with MDD (Figure 2).
When compared with the Hanley and McNeil’s test, the MDQ was confirmed better than the HCL-32 in distinguishing patients with BD from putatively healthy controls, while no difference was found between the two screeners in the differentiation of patients with BD from those with MDD (Figure 3).
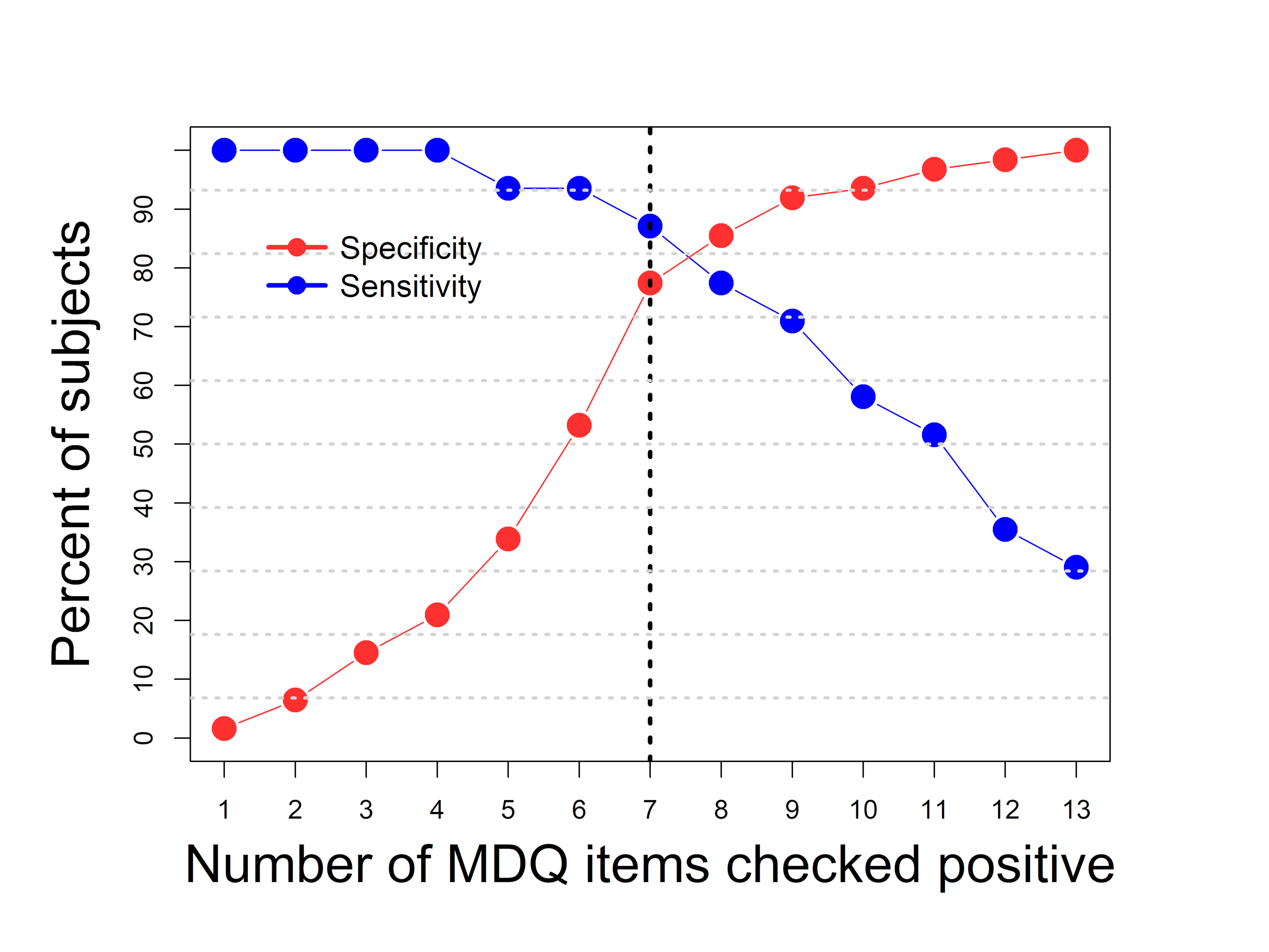
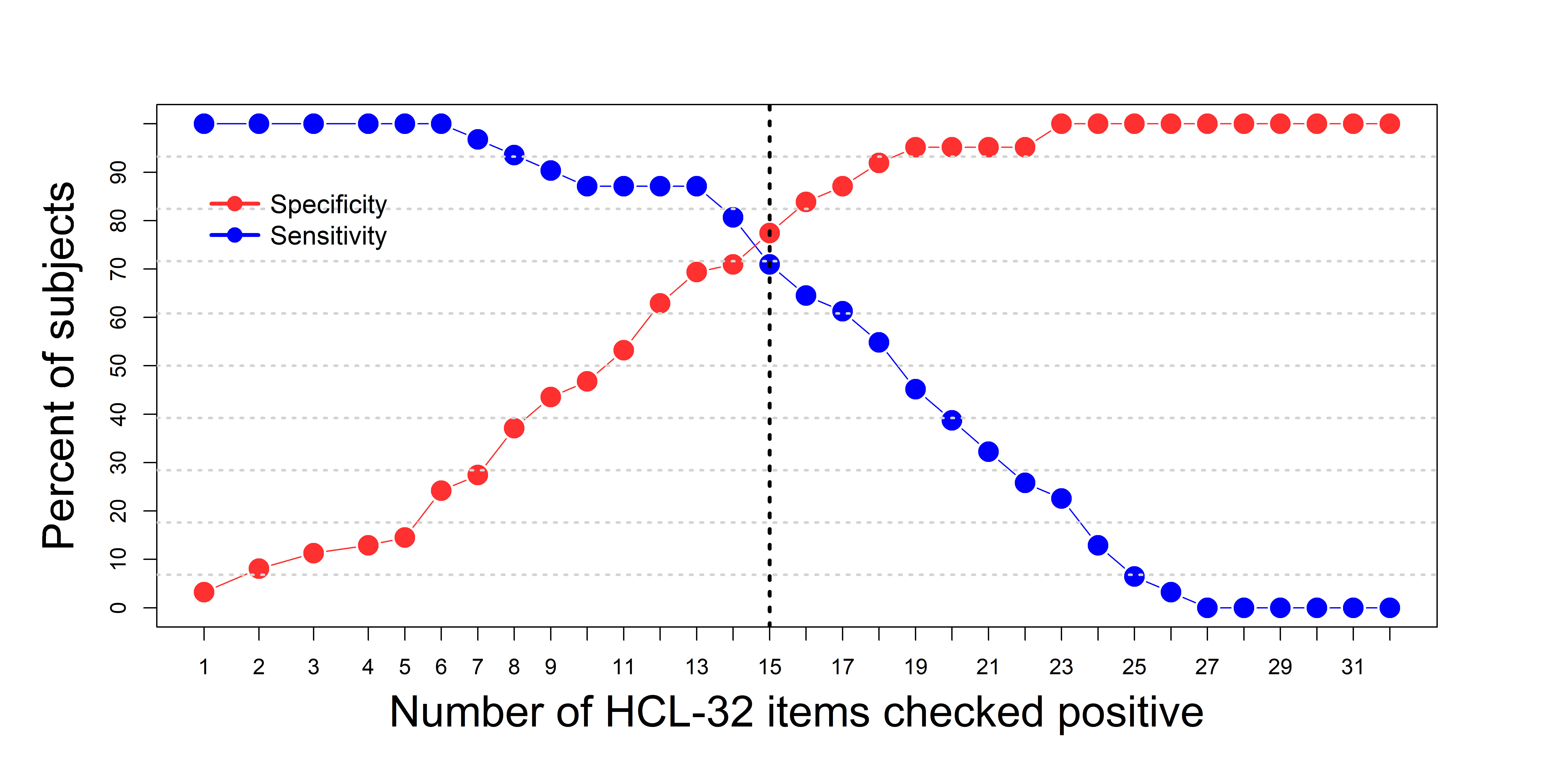
The best threshold for the differentiation of patients with BD from patients with MDD was 7 for the MDQ (Figure A1) and 15 for the HCL-32 (Figure A2).
Sensitivity and specificity at the best threshold were 87% and 77%, respectively, for the MDQ, and 87% and 69% for the HCL-32. Both screeners had a better NPV (92.3% and 91.4%, respectively) than PPV (65.8% and 58.7%). The positive diagnostic likelihood ratio was modestly higher for the MDQ (3.86) than for the HCL-32 (2.84).
In the investigated samples, 109 controls (41.1%), 21 patients with MDD (24.4%), and 52 patients with BD (89.7%) scored at or above the cut-off on the MDQ (÷2=63.14; df=2; p<0.0001). The corresponding figures for the HCL-32 were 108 (48%) among controls, 21 (32.8%) among patients with MDD, and 28 (87.5%) among patients with BD (÷2=25.78; df=2; p<0.0001).
{kind=link}
{kind=link}