After collecting the data in the basic excel table, they were processed with the aim of displaying the results of the study according to the tables below.
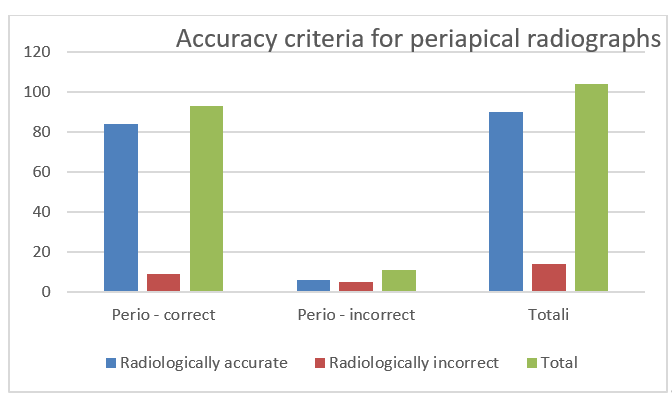
Table 1. Division of radiographs depending on the fulfillment of the criteria for accurate radiography.
|
X-rays
|
Radiologically accurate
|
%
|
Radiologically incorrect
|
%
|
Total -%
|
|
Perio - correct
|
84
|
81%
|
9
|
9%
|
93-89%
|
|
Perio - incorrect
|
6
|
6%
|
5
|
5%
|
11-11%
|
|
%
|
90-87%
|
87%
|
14-13%
|
14%
|
104-100%
|
Based on the criteria for an accurate periapical radiograph that can be used for periodontal evaluation of the tooth in table 2 and graph 2 are presented periodontally incorrect graphs depending on which criteria they were evaluated as incorrect.
Table 2. Table 2 shows the error of periodontal radiographs depending on which criterion this error is.
|
Patients
|
No. of X-rays
|
% of error
|
% of coverage
|
% of coverage
|
% of coverage
|
|
Criterion 1
|
11
|
100%
|
18%
|
8-72%
|
9- 82%
|
|
Criterion 2
|
2
|
18%
|
2-18%
|
|
Criterion 3
|
6
|
55%
|
55%
|
|
Criterion 4
|
-
|
0%
|
0%
|
0%
|
|
Total
|
19
|
170%
|
73%
|
72%
|
100%
|
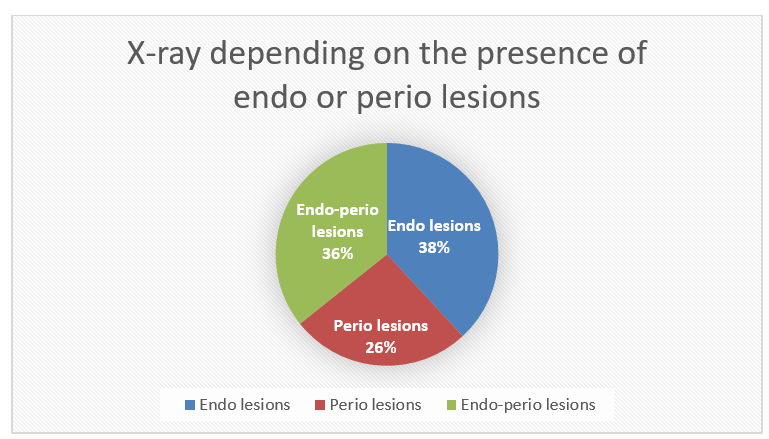
Table 3. Table 3 shows the distribution of radiographs depending on the presence of endo or perio lesions.
|
X-rays
|
Nr.
|
%
|
|
Endo lesions
|
32
|
38%
|
|
Perio lesions
|
22
|
26%
|
|
Endo-Perio lezions
|
30
|
36%
|
|
Total
|
84
|
100%
|
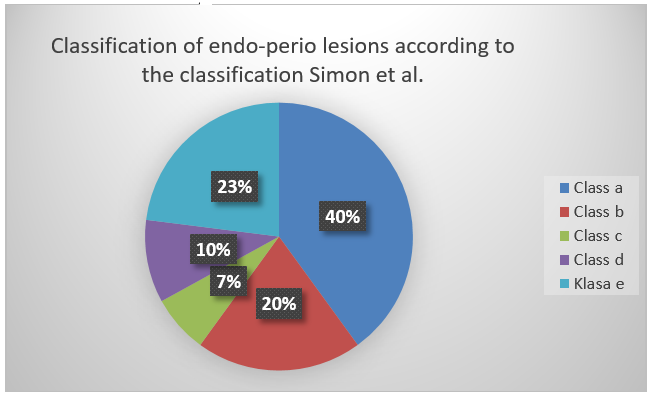
Table 4. The table summarizes the data of the radiographs for the classification of endo-perio lesions according to the classification Simon et al.
|
X-Rays
|
No.
|
%
|
|
Class a
|
12
|
40%
|
|
Class b
|
6
|
20%
|
|
Class c
|
2
|
7%
|
|
Class d
|
3
|
10%
|
|
Class e
|
7
|
23%
|
|
Total
|
30
|
100%
|
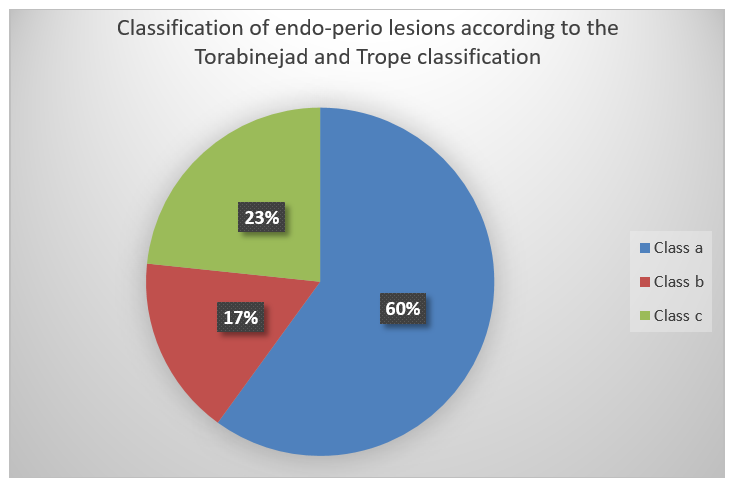
Table 5. The table summarizes the radiographic data for the classification of endo-perio lesions according to the Torabinejad and Trope classification.
|
X-rays
|
No.
|
%
|
|
Class a
|
18
|
60%
|
|
Class b
|
5
|
17%
|
|
Class c
|
7
|
23%
|
|
Total
|
30
|
100%
|
Figures 1-6 show some of the patients included in the study.
Periapical radiographs should be evaluated initially for their accuracy, both for radiographic and periodontal criteria. The protocol for the routine performance of periapical radiographs requires accuracy in the positioning of the cone in the superior-inferior direction or even in the mesial-distal direction, mainly if we evaluate the radiographs for accuracy according to the Prichard criteria. These criteria do not allow for misplacement of the radiograph cone, an element that is checked several times in different angles according to Prichard's criteria. Going beyond these criteria is included in criterion 1, which categorically prohibits the top-down displacement of the cone, and then criterion 4 strengthens criterion 1 even more, not allowing any minimal violation in the positioning of the radiograph cone. Criterion 2 and criterion 3 are in line with each other, orienting around the positioning of the cone and its movement to the left or right. This is often reflected in the coverage that the teeth make at the point of contact, which should be empty, so there are no tooth clusters.
Part of the selection of accurate radiographs, both periodontally and radiographically, helps us to examine endo lesions, perio lesions, and combined endo-perio lesions as accurately as possible.(7,12,15,18,23,25,37,43)
The presence of endo-perio lesions is one of the reasons why the tooth may go to extraction. The combination of the lesion of perio origin to pass to the endo lesion, or vice versa the endo lesion to pass to the perio lesion, leads to the combination of the bacterial flora causing the inflammation which finds a communication path between the tooth-bearing structures and the pulp structure. Depending on the area where the lesion appears, the objective and subjective complaints of the lesion presented and referred by the patient may be combined. Differential diagnosis in the appearance of objective and subjective complaints should be performed carefully, prioritizing the use of accurate periapical radiography.(2,15,24,38,42-49)
Endo-perio lesions have been subjected to various classifications, modified over time. At the moment when this classification is an integral part of a larger classification such as the classification of periodontal diseases, changes in the classification of periodontal diseases consequently pass and express changes in the classification of personalized endo-perio lesions.(12,35,37) Many authors have copyrighted their proposed endo-perio classifications. It is important that the classification of endo-perio lesions is performed on the basis of radiographic data and the transition from one subclass to another is very sensitive and specific according to apparently minimal radiographic changes of the affected structures. A significant coverage of some subclasses of one classification to a subclass of another classification is distinguished. This coverage requires even higher radiographic accuracy and precise knowledge to determine the criteria when a lesion belongs to a subclass of the classification and when this lesion passes with its characteristics to the next subclass. (15,16,27,38,39,40,43-49)
Each classification or subclass of the general classification of endo-perio lesions enables orientation on the treatment of the lesion, in the sense of which of the therapies is primary, that of the endodontic treatment of the tooth, or that of its periodontal treatment.(34,35,41)
The true combined endo-perio lesion with high vulnerability of the tooth furcation, that is, the lesion presented in the molars, has a prognosis that also leads to tooth extraction, since the vulnerability of the tooth-bearing structures is high and their renewal requires periodontal surgical procedures biasing somewhat against tooth hemisection procedures, or extraction of the affected tooth.(33,34,36)
As results expressed in figures, documented by our study, they are as follows:
- Classification of radiographs based on whether they met accuracy criteria showed that 81% of radiographs met periodontal and radiographic criteria simultaneously. 9% were perioperatively and radiologically incorrect; perio incorrect and radiologically correct were in 6% and recently both evaluation criteria were incorrect in 5% of the included cases.
- For periodontal criteria on the accuracy of radiographs: 100% did not fulfill Prichard's criterion 1, 8% did not fulfill Prichard's criterion 2, 55% did not fulfill criterion 3 and 0% was related to fulfilling criterion 4.
- The percentage of coverage in non-fulfillment of criteria 1 and 2 was 18%. The coverage percentage of the 3rd criterion and the 4th criterion was 55%. The percentage of coverage of criterion 1,2 and 3 was simultaneously at 72%. Non-fulfillment for criterion 4 was at the value of 0%. The average percentage of coverage for the four criteria was about 73%.
- The distribution of radiographs depending on the presence of endo or perio lesions varies as follows: endo lesions were presented in 32 cases or in 38% of the radiographs; perio lesions were present in 22 cases or in 26% of the radiographs and endo-perio lesions were in 30 cases or in 36% of the radiographs included in the study.
- According to the classification Simon etal. radiographs were divided: class a 40%, class b 20% class c 7% class d 10% and class e 23%.
- According to Tobabinejad and Trope classification, endo-perio lesions were according to classes specifically: class a 60% class b 17% class c 23%.
{kind=link}
{kind=link}
{kind=link}
{kind=link}