4.1. Prevalence rate
The Global Burden of Disease (GBD)-2019 has revealed that headache prevalence is much higher in the top economically developed nations, with the greatest prevalence rates being observed in Italy (49.02%) and the USA (45.11%). Regarding the India’s neighbouring countries and the states of India, the highest prevalence has been recorded in Sri Lanka (37.2%) followed by Nepal (35.95) and the states of Sikkim (38.08%) and Goa (35.24%) respectively (Global Burden of Disease (GBD)-2019).
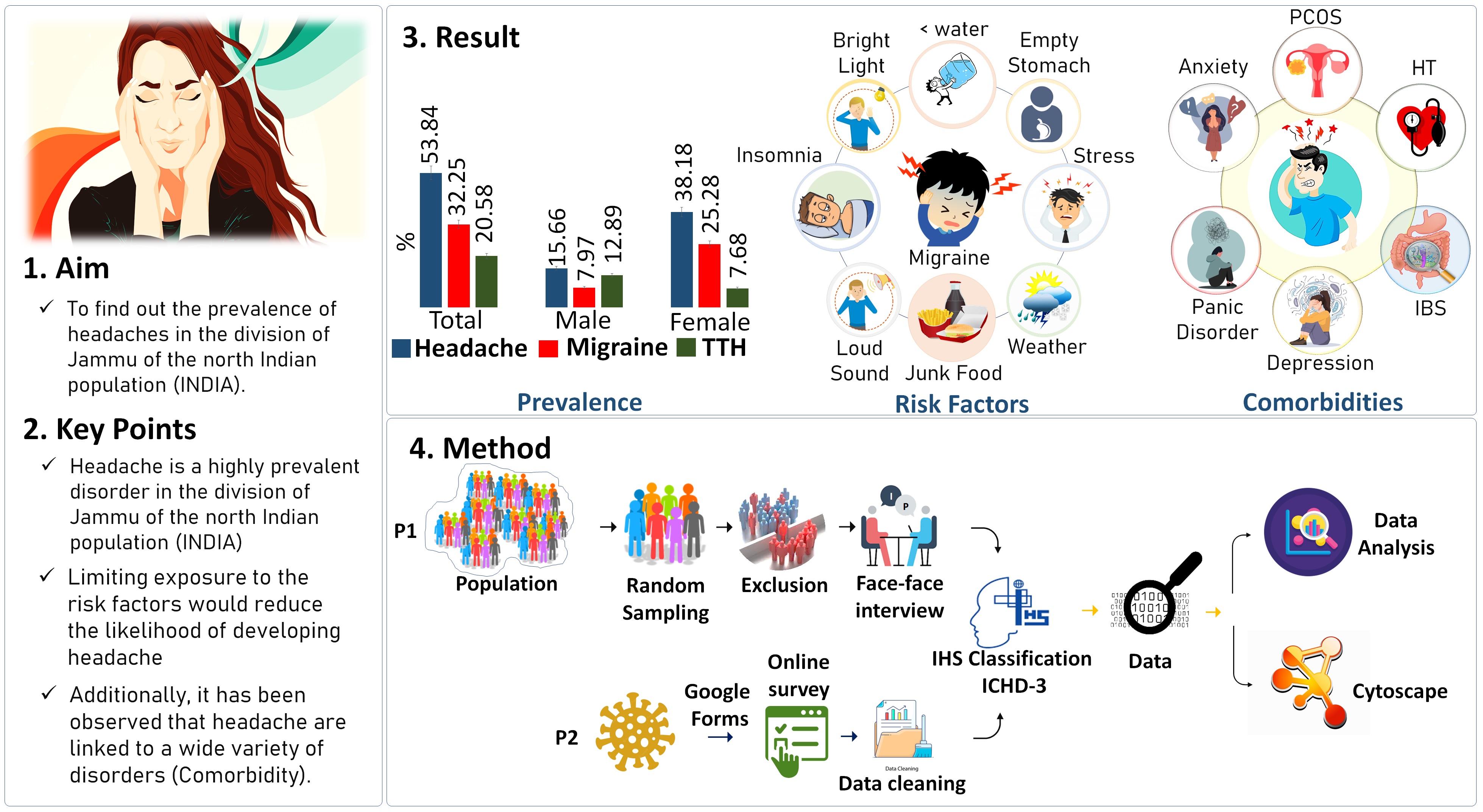
In the current study, high headache prevalence estimates were found (Fig. 3) which is also consistent with the other epidemiological study conducted in different regions of India. In south India, headache prevalence is 63.9% with a female preponderance of 73% in comparison to male (54.4%), TTH is 34.8% and migraine 25.6% (female:32.4% & male: 18.6%) (Kulkarni et al., 2015). In the eastern states of India, headache prevalence was 14.87% where the females were 23.51% and males were 5.44 and migraine was 14.12% (males: 5.35% and 22.16%) (Ray et al., 2017). In the north Indian region, different studies have shown that the headache prevalence is 63.9% wherein females were found to be more affected (74.3%) as compared to males (32.6%). Prevalence of migraine was 13.44% with a female preponderance (87.5%) (Nandha et al., 2013). A prospective observational study in the north Indian population found that 67.7% of patients had migraine and 32.2% of patients had tension-type headaches (TTH) (Sastry et al., 2022). In the valley of Kashmir, headache in the pediatric population was observed where the frequency was found at 66.4% with the female at 65.15% and male at 35.85%, Migraine at 26.98%, and TTH at 50.99% (Malik et al., 2012). Another group found the headache frequency rate equal to 66.20% (19–45 years) with female dominancy (61.82%) to male (38.18%). In migraine, the total prevalence was found 45.69% with 55.44% in females and 32.0% in males (Masoodi et al., 2016).
To this end, the prevalence of headache and its type varies from region to region and this disparity is mighty due to the different sampling approach (simple random, clustered, stratified sampling), different sample size, type of study (population-based/ hospital case-control, cohort), the differing methodology adopted, differences in defining the criteria of headache prevalence (1 year vs. 3 months), coexisting environmental factors, urban/rural differences, or ethnicity of the studied population.
4.2. Environmental risk factors
Headaches were strongly connected with concurrent disorders, routine drug use, analgesic use for diseases other than headaches, and a variety of environmental risk variables (Nieswand et al. 2019). In the present study, different environmental factors have been observed which increase the risk of condition significantly (Fig. 4).
In the present study, bright light was found significantly (p < 0.0001) associated with headache (OR: 5.81) and various studies have supported the fact that bright light within the range of 450 nm to 578 nm wavelength significantly alter the condition (Drummond, 1986; Main et al., 2000; Ofovwe & Ofili, 2010). Bright light significantly excites the nociceptive neurons in superficial laminae of trigeminal subnucleus caudalis (Vc/C1) mediated by an intraocular mechanism and transmission through the TRG (Trigeminal root ganglion) (Okamoto et al., 2010) and responsible for pain (Moulton et al., 2009). Bright light also modulates the dura-sensitive neurons in the posterior thalamus whose axons are projected extensively across layers I–V of somatosensory, visual, and associative cortices. The cell bodies and dendrites of such dura/light-sensitive neurons were opposed by axons originating from retinal ganglion cells (RGCs), predominantly from intrinsicality photosensitive RGCs (Retinal Ganglion Cells) (Noseda et al., 2010). Other than the classical pathways, a research study has also supported the other non-classical pathway mediated through the melanopsin, a photopigment that underlies subconscious vision, in the trigeminal nerve (Matynia et al., 2016). CGRP (Calcitonin Gene Related Peptide), a potent vasodilator has been found to mediate the transfer of bright light stimulus and anti-CGRP or vasoconstrictive agents blocked light-evoked neural activity (Okamoto et al., 2010; Navratilova et al., 2019).
Weather is another interesting risk factor that have been found to be a profound risk attribute of headaches, as we have also observed that different weather conditions significantly increase the likelihood of headaches (See Result section). In support of our study, other studies have shown that weather changes act as a trigger for headache onset or the worsening of ongoing headache symptoms (Prince et al., 2004). Lower temperature and higher relative humidity have been significantly associated with the onset of a migraine period (Hoffmann et al., 2011). Increases and decreases in temperature lead to a significant increase in the number of migraine attacks (Scheidt et al., 2013). Temperature change accounted for 16.5% of the variance in headache incidence in winter and 9.6% in summer (Yang et al., 2015). This high variance is due to the variance for the temperature and sunshine duration, followed by humidity and pressure during cold (Yang et al., 2011).
TRPM8 (Transient receptor-potential M8), a cation channel (Na+ and Ca++) is the prime candidate for temperature sensation and is expressed in pain sensory neurons (McKemy et al., 2002) Genome-wide association studies (GWAS) have implicated the TRPM8 channel in association migraine (Hautakangas et al., 2022) and it has been found that decreased expression of TRPM8 is associated with a reduced risk for migraine where homozygous carriers of rs10166942[C] were less sensitive to cold pain (McKemy et al., 2002).
Stress can be physiological and oxidative wherein physiological stress includes social support, loneliness, marriage status, social disruption, work environment, social status, social integration, etc, and oxidative represents the increased reactive oxygen species and reactive nitrogen species in the blood. Other than oxidative, physiological stress has greatly influenced the headache where it is found that an increase in the stress intensity will increase the headache frequency (Schramm et al., 2015). Different forms include occupational stress (Lin et al., 2007; Gillespie et al., 2015; Godwin et al., 2016), educational stress (Ghorbani et al., 2013; Ibrahim et al., 2017) have been found to be associated with headaches.
Sleep quality is closely linked to headache (Yokoyama et al., 2019), which affects around 30–50% of migraine patients, and is one of the reasons why migraine sufferers are prone to morning headaches because of sleep deprivation. The impact of sleep disturbances increases self-reported pain and leads to a disturbance of the descending pain inhibitory control system (Lin et al., 2016; Negro et al 2020).
Another important risk factor that was found to be significantly associated with the condition was less water intake (See Result Section). In support of our study, various studies have found that water deprivation may play a role in migraine, particularly in prolonging attacks (Blau et al., 2004), and drinking more water resulted in a statistically significant improvement (Price & Burls, 2015). This water ingestion provided relief from headache within 30min to 3hr. It is proposed that water deprivation-induced headache is the result of intracranial dehydration and total plasma volume (Popkin et al., 2010). Studies have also shown that water intake did not affect the number of headache episodes, but was associated modestly with a reduction in headache intensity and reduced duration of headache (Spigt et al., 2005). Despite such benefits of water intake, it has also been shown that headache is also caused by drinking cold water which is called “ice-water stimulus provoked headache” attributed to ingestion or inhalation of a cold stimulus (Mages et al., 2017) and this pain perception is induced by a cold palatal stimulus (Mattsson, 2001; Mages et al., 2017). There has been also reported that there has a negative correlation between water intake and the frequency of headaches. (Khorsha et al., 2020).
The most extensively used psychostimulant substance in the world is caffeine, also known as trimethylxanthine, an alkaloid that occurs naturally in several plants. The current study provides insight into the risk-attribution potential of caffeine by demonstrating its modest risk capability which significantly (p < 0.0001) increases the chance of condition by 1.95fold. In support of our study, population-based cases and controls have found that patients with chronic daily headache (CDH) were more likely overall to have been high caffeine consumers before the onset of CDH (Scher et al., 2004). Also, a prospective cohort study, conducted by Mostofsky and the group found that high levels of caffeinated beverage intake may be a trigger of migraine headaches (Mostofsky et al., 2019). It has also been shown that the sudden cessation of caffeine use after chronic exposures leads to a withdrawal syndrome with headache as a dominant symptom (Shapiro, 2008), constipation, impaired behavioural and cognitive performance, joint pains, decreased or increased blood pressure, increased heart rate, hand tremor, increased diuresis, and abdominal pain (Juliano & Griffiths, 2004; Meredith et al., 2013).
But in contrast to its risk attribution, with intermittent exposure, caffeine may act as a mild analgesic for headache or as an adjuvant for the actions of other analgesics (Shapiro, 2008). The doses of 130 mg enhance the efficacy of analgesics in TTH and doses of ≥ 100 mg enhance benefits in migraine (Lipton et al., 2017). It is not recommended to exceed 400–450 mg/day, because chronic repetitive exposures to caffeine increase the risks for the development of analgesic-overuse headache, and chronic daily headache (Hering-Hanit & Gadoth, 2003). Caffeine is rapidly and completely absorbed into the bloodstream after oral ingestion, with peak blood levels reached in 30 min to 45 min. Caffeine with a typical half-life of four to six hours is metabolized by the liver and is excreted by the kidneys via urine (Meredith et al.2013). Caffeine molecules are structurally similar to adenosine and bind to adenosine receptors on the cell surface and act as competitive inhibitors. As the inhibitory effect of caffeine on adenosine receptors, the state of cortical hyperexcitability is established and this increases alertness and improves cognitive function (Espinosa Jovel & Sobrino Mejía, 2017). Also, caffeine releases dopamine and stimulates glucose utilization in the prefrontal cortex and a caudate nucleus respectively which help in positive reinforcement and mediates motor activity and regulate the sleep-wake cycle respectively (O'Callaghan et al., 2018).
We also observed that empty stomach/ fasting significantly (p < 0.0001) increases the likelihood of headache by 3.42fold, which is also supported by various epidemiological studies (Bánk & Márton, 2000; Abu-Salameh et al., 2010). The length of the fasting-induced headache is dependent on the length of the fast and pain is featured as non-pulsating, mild to moderately intense, wide, or centred in the frontal area (Torelli & Manzoni, 2010). The fact has also been supported that after a long time if an individual takes a meal, the chance of postprandial fasting-related headaches increases which is featured with episodic in nature, heaviness (AlAmri et al., 2021). The proposed mechanism depicts that a network of neurons and astrocytes may collectively depolarize as a result of an imbalance between the excitatory and inhibitory processes set by a lack of glycogen-derived glucose at the start of intensive synaptic activity. Activating pannexin1 channels in neurons and starting parenchymal inflammatory pathways, may stimulate perivascular trigeminal afferents (Dalkara & Kilic, 2013).
In addition, dietary habit such as consumption of red meat/ non-vegetarian food was not found significantly ((p = 0.9487) associated with headache but on the other hand junk food, dairy products (such as milk, curd, ice-creams, etc.) significantly associated with the condition with an OR: 1.95, 95% CIs [1.69–2.25] (p < 0.0001), OR: 1.36, 95% CIs [1.14–1.62] (p = 0.0006). Regarding diary products conflicting result have been reported (Mansouri et al., 2020) and patients with migraines consumed less milk than people without migraines (Nazari & Eghbali, 2012; Rist et al., 2015).
Enclosing the section, the present epidemiology study has presented a various range of environmental risk attributes that significantly increases the likelihood of headache. Patients with headaches need to be enlightened about the risk factors that contribute to their condition so that they can avoid them and possibly reduce their headache frequency.
4.3. Comorbidities
Co-morbidity is another great thing of concern that needs to be thought about and is defined as the presence of two or more chronic conditions at the same time (Valderas et al., 2009). Comorbidity with headache is a common concern, with more than a third of patients seen by primary care physicians having four or more chronic health issues, and a small percentage having more than ten.
In the present epidemiological study, various condition has been found to be associated with headache (Fig. 5). As in the present study, IBS was found to be highly associated with headache {OR: 3.8084, 95% [1.7610–8.2360] (p = 0.0007)}. Different epidemiological research from different parts of the world has shown the high rates of co-existing IBS and headache which supports our research (Chang & Lu, 2013; Lau et al., 2014; Mirzaei et al.,2016; Li et al., 2017; Kawashima et al., 2020; Grover et al., 2021). Headache sufferers specifically migraineurs with long headache history and high headache frequency have a higher chance of being diagnosed with IBS. IBS and migraine share some similarities and can alter gut microflora composition and thereby may affect the gut-brain axis and inflammatory status (Arzani et al., 2020). A key neurotransmitter i.e., serotonin plays a role in both conditions, wherein IBS serotonin causes excessive bowel motions, a lot of digestive output, as well as visceral hypersensitivity in the gut, and defective serotonin activity in the central nervous system is responsible for the migraine. (Camilleri, 2009). In addition, individuals with IBS and migraine have been found to have high family aggregation and genetic variations, such as those in the serotonin reuptake transporter gene (5-HTTLPR) (Schürks et al., 2010; Zhang et al., 2014).
Other than IBS, PCOS was also found to be significantly (p < 0.0001) associated with headache (OR: 8.6336). Different studies have shown that women with PCOS are burdened with multimorbidity which includes hypertension, tendinitis, osteoarthritis, fractures, endometriosis, and importantly migraine (Glintborg et al., 2015; Banday et al., 2022 Kujanpää et al., 2022). The PCOS-disease subnetworks were subjected to pathway enrichment analysis and found a substantial relationship between PCOS and other illnesses like hypertension and migraine (Ramly et al., 2019). Other conditions like anxiety, hypertension, depression, and panic disorder are also comorbid conditions associated with the headache (Muayqil et al., 2018; Caponnetto et al., 2021; Togha et al., 2022) including uric acid and (Yazar et al., 2021) and hypothyroidism (Lima et al., 2017; Rubino et al., 2019; Spanou et al., 2019). Increased levels of uric acid and serum cholesterol have been reported to strongly correlate with white matter hyperintensities; this association may be explained by altered endothelial dysfunction and increased attack frequency (Trauninger et al., 2011).
Comorbidity of diseases with headaches may be due to several reasons some of which include sharing common pathophysiological mechanisms (Lauritzen et al., 2011), common risk factors including the common genetic variants, and common environmental risk factors. Comorbidity with common diseases is mostly concerned with the sharing of common risk attributes which are frequently used whether it is genetic or environmental factors.
{kind=link}