The antigens present in human red blood cells are a collection of glycoproteins and glycolipids. These antigens are genetically regulated, appearing early in fetal life and remain unaltered until death. The most important blood group antigen after ABO, and Rh is the Kell blood group described in different ethnic groups [1]. Coomb, Race, and Mourant discovered the Kell blood group system from a child of Mrs. Kellacher who had the hemolytic disease in a newborn, and the search for antigen led to the finding of a new antigen, which was dubbed "Kell" [2]. This blood group is ranked the third number of all blood group systems discovered yet, owing to its involvement in immunological reactions. It consists of a single 93 kDa red-cell transmembrane protein that usually carries 36 antigens [3].
The Kell protein consists of 732AA that are glycosylated at five different locations and pass through the membrane of RBC. This protein is associated with another transmembrane protein XK, which anchors it to the RBC surface by a disulfide linkage. McLeod's syndrome develops due to the absence of XK protein. XK protein is a zinc-dependent endopeptidase that cut proteins within the peptide chain and shares sequence and structural similarities with the Kell protein. For catalysis and zinc-binding a pentameric region is required that is found in this protein and other members of this family [4].
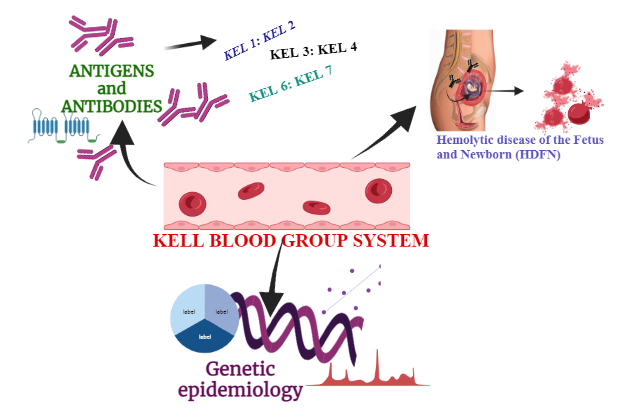
The gene of this protein is found at chromosome 7q33 and have19 exons encompassing more than 20kb of genomic DNA [5]. The SNP (C578T) in exon 6 induces alteration from Threonine to Methionine at 193 positions, resulting in the KEL1 and KEL2 antigens (in the K antigen). A mutation (C841T) in exon 8 resulted in an R281W alteration in KEL3 and KEL4 antigens. A single nucleotide polymorphism (T1790C) in KEL6 which code for proline at position 597, may result in KEL7 antigens, where it codes for leucine (Fig.1), [6].
The common genotypes of Kell blood group system are K+k+, K+k-, K-k+, Kp (a-b+), Kp (a+b+), Kp (a+b-), Js (a+b+), Js (a-b+), Js (a+b-). Out of these, K-k+, Kp (a-b+) and Js (a-b+) have high incidence ratio while K+k+, K+k, Kp (a+b+), Kp (a+b-), Js (a+b+), and Js (a+b-) are low frequency genotypes (Table: 1), [7].
Kell Antigens
In this blood system, 27 antigens are present although only Kell (K1) and cellano (K2) are clinically important. After ABO and Rh antigens, they may be immunogenic since they have been linked to severe hemolytic disease in newborns [8]. Kell antigens are grouped in antipodal set pairings with some antigens that have yet to find antithetical partners [9]. KEL1 (K, "Kell") and KEL2 (k, "Cellano"); KEL3 (Kpa), KEL4 (Kpb), and KEL21 (Kpc); KEL6 (Jsa) and KEL7 (Jsb) are antithetical antigens [10]. KEL4 in contrast to other common antigens is linked to two antithetical antigens KEL3 and KEL21 [9]. Individuals with negative KEL2, KEL4, or KEL7 antigens have uncommon phenotypes, Ko (null) phenotype is present in individuals in which all Kell antigens are absent [11]. The table 1 below expresses the total antigens, their names, notation, and their antigenic frequency.
Table 1: Antigens in KELL Blood Group
|
ISBT No.
|
Notation
|
Names
|
Exon
|
AA* Change
|
Frequency
|
References
|
|
KEL1
|
K
|
Kell
|
6
|
T 193 M
|
~2 - 25%
|
[12]
|
|
KEL2
|
K
|
Cellano
|
11
|
A 423 V
|
~100%
|
[13]
|
|
KEL3
|
Kpa
|
Penny
|
8
|
Arg 281 Trp
|
~1.99%
|
[14]
|
|
KEL4
|
Kpb
|
Rautenberg
|
-
|
-
|
~100%
|
[15]
|
|
KEL5
|
Ku
|
(K0)
|
|
|
~100%
|
[15]
|
|
KEL6
|
Jsa
|
Sutter
|
17
|
Leu 597 Pro
|
~0.01%
|
[16]
|
|
KEL7
|
Jsb
|
Metthews
|
-
|
-
|
~100%
|
[15]
|
|
KEL8
|
Kw
|
-
|
-
|
-
|
~5%
|
[15]
|
|
KEL9
|
KL
|
Claas
|
-
|
-
|
~100%
|
[15]
|
|
KEL10
|
U1a
|
Karhula
|
13
|
Glu 494 Val
|
~2%
|
[14]
|
|
KEL11
|
-
|
Cȏté
|
-
|
-
|
~100%
|
[15]
|
|
KEL12
|
-
|
Bockman
|
15
|
His 548 Arg
|
~100%
|
[13]
|
|
KEL13
|
-
|
Sgro
|
-
|
-
|
~100%
|
[15]
|
|
KEL14
|
|
Santini
|
-
|
-
|
~100%
|
[15]
|
|
KEL15
|
Kx
|
-
|
-
|
-
|
~100%
|
[15]
|
|
KEL16
|
-
|
-
|
-
|
-
|
~100%
|
[15]
|
|
KEL17
|
Wka
|
Weeks
|
8
|
Val 302 Ala
|
~0.3%
|
[14]
|
|
KEL18
|
-
|
Marshall
|
4
|
Arg 130 Trp
|
~100%
|
[13]
|
|
KEL19
|
-
|
Sublet
|
13
|
Arg 492 Gln
|
~100%
|
[13]
|
|
KEL20
|
Km
|
-
|
-
|
-
|
~100%
|
[15]
|
|
KEL21
|
Kpc
|
Leves
|
8
|
Arg 281 Gln
|
~0.01%
|
[14]
|
|
KEL22
|
-
|
Ikar
|
9
|
Ala 322 Val
|
>99.9%
|
[13]
|
|
KEL23
|
-
|
-
|
10
|
Gln 382 Arg
|
~0.01%
|
[13]
|
|
KEL24
|
-
|
Clas
|
6
|
Arg 180 Pro
|
< 0.2%
|
[13]
|
|
KEL25
|
-
|
VLAN
|
-
|
-
|
Rare
|
[15]
|
|
KEL26
|
-
|
TOU
|
11
|
Arg 406 Gln
|
~100%
|
[13]
|
|
KEL27
|
-
|
RAZ
|
-
|
-
|
~100%
|
[15]
|
*AA stands for Amino acids
Kell Antibodies and Transfusion Reaction
Antibodies that target Kell antigens are commonly IgG that are anti-K1, anti-K2, anti-K3, and anti-K7 that become the cause of hemolytic disease in newborns and transfusion reaction [4]. The K1 antibody (anti-K1) is responsible for severe anemia in 10% of cases [17]. The lesser number of cases are caused by anti-K2 [18], anti-K3 [19], anti-K6 [20], and anti-K7 [21] which have been associated with HDFN. Literature reports of the frequency of hemolytic transfusion reactions and the resulting mortality rate of 1/76,000 have been observed [18, 22].
Common Phenotypes Associated with Kell
1 Hemolytic Transfusion Reaction
The hemolytic transfusion reaction is caused by alloimmunization after transplantation and packed red blood cells (RBCs) transfusions [23]. Transfusion reasons may be mild to severe. These reactions may occur immediately after blood transfusion known as acute transfusion or maybe later after many weeks known as delayed transfusion [24]. The Anti-K, anti-Kpa, anti-k, and Anti-Js1 antibodies are responsible for producing a more lethal transfusion reaction [4]. In people with the K0 phenotype, the production of Ku antibodies led to a lethal transfusion reaction [25].
2 Hemolytic Disease of Fetus and Newborns
Antibodies formed as a result of Kell antigen can trigger transfusion reactions and neonatal hemolytic illness (HDN). It usually affects women who have had multiple blood transfusions, but it can also affect moms who had sensitization to Kell antigen in early gestation. Kell sensitization, unlike Rh and ABO hypersensitivity, is produced by anti-K antibodies limiting RBC synthesis in the fetus. Kell antigens are present in the peripheral area of RBC precursors by the tenth week of life, and Kell antibodies promote the macrophages that cause immune destruction of progenitor cells in the liver of the fetus. Since RBC precursors are devoid of Hb, a small quantity of bilirubin is mixed in amniotic fluid during the hemolysis, and anti-Kell antibodies cause fetal anemia by destroying fetal erythroid progenitors [26, 27].
Erythropoiesis is the development of mature red blood cells from erythroid progenitor cells [28]. During early erythropoiesis, the expression of Kell glycoprotein is high implying a key function in the early phases of erythropoiesis [29]. At the progenitor level, Maternal Kell antibodies decrease erythropoiesis in fetuses which lowers the number of reticulocytes associated with severe anemia as well as reduced bilirubin [30]. Kell alloimmunization may cause severe anemia and hydrops in newborn babies, due to early cell death before red blood cells collect sufficient hemoglobin levels (Fig:2), [31].
Uncommon Phenotypes Associated with KEL
KEL gene is highly polymorphic that encodes many KEL proteins.
1 Null Phenotype
Ko is an uncommon null phenotypic trait in the Kell system caused by a variety of KEL mutations, like improper splicing, nucleotide deletion, and premature stop codons, where Kell antigens are not present on RBCs. The health status of such phenotypic persons is good but when they come into contact with RBCs that contain Kell antigens, they create anti-Ku. Anti-Ku is associated with moderate to severe forms of transfusion reaction, resulting in the death of individuals possessing this phenotype. So, if a Ko person needs a blood transfusion, it is recommended to use only Ko blood components [32].
2 KMOD Phenotype
Kmod is a hereditary RBC phenotype defined by low but detectable expression of Kell antigens with a high incidence [33] . Four Kmod phenotypes Kmod-1 (1208G>A), Kmod-2 (2150A>G), Kmod-3 (1106T>C), and Kmod-4 (2227G>A) of were identified [34].
3 McLeod Phenotype
The Kell protein is chemically bonded to the XK protein which is hypothesized to perform the function of transportation, in the membrane of red blood cells [35]. When XK is missing, a disease known as McLeod syndrome develops, in which Kell antigens give very light expression and erythrocytes have abnormal spiny extensions (acanthocytosis). Muscular dystrophy, heart problem, mental abnormalities, and nervous system impairments such as malfunction of reflexes and balance abnormality are among the main results [36].
{kind=link}