In an era where the average lifespan extends beyond 90 years in many regions of the world, there is an increased demand for improvements in quantity and quality of life. In this context, regenerative medicine is a field of great importance. Awareness of various blood-borne diseases has raised concerns over perioperative transfusions, with no exception to the field of OBGY. Exposure to multiple allogeneic blood transfusions also results in precipitation that induces the formation of irregular antibodies.
Various conditions occurring in women during the reproductive phase frequently involve acute and chronic anemia, and appropriate red blood cell replacement is a vital aspect of conservative and perioperative management. The World Health Organization (WHO) reported that approximately 118.4 million blood donations are collected worldwide in 2018.(23) Approximately 40% of these are collected in high-income countries accounting for 16% of the world’s population. The risk of transmission of serious infections, including HIV and hepatitis, through unsafe blood transfusions and a worldwide trend of chronic blood shortage has attracted global attention to the safety and availability of usable blood and blood products. With the goal of ensuring universal access to safe blood and blood products, the WHO has issued specific integrated strategies for blood safety and availability. With the increase in blood-borne infectious diseases and aging population in many regions, the number of candidates eligible for blood donation is decreasing. Hence, the discovery of an alternative source of anemia treatment that is safer than allogenic transfusion, and more efficient and faster than iron replacement, is needed.
In the clinical setting, endometrial tissues obtained after hysterectomy could be alternatively obtained through endometrial biopsy, which is minimally invasive and non-scar forming. The hypothesis that innate multipotent cells exist within the endometrium and that its plasticity will serve as an excellent source for reprogramming has been investigated in a few studies. More in-depth studies including directed differentiation using endometrium-driven cell sources are scarce. The merit of inducing erythroid differentiation using recycled post-surgical endometrial tissue, when stored in the form of iPSCs, is that the source is abundant, versatile and could be alternatively used for other on-demand tissue engineering purposes. Moreover, because mature red blood cells are enucleated, differentiated RBCs of iPS cell origin could be a suitable candidate for cell therapy with low concern for ectopic gene integration associated with iPSCs.
Yamanaka et al., who first reported iPSC derived from murine fibroblasts in 2006,(5) was awarded the Nobel Prize in Medicine only six years after the first description, in recognition of the potential of iPSCs for regenerative medicine and disease modeling. Reprogrammed stem cells are attracting attention not only in the production of next-generation immune-compatible stem cell therapeutics, but also as models for identifying disease etiology, therapeutic efficacy, and toxicity testing.(24) Recently, iPSCs have gained attention as precursor cells for organoid research.(25) An additional advantage of iPSCs is the exemption from ethical issues encountered with embryonic stem cells, while their differentiation potential to different lineages is considered pluripotent.
The idea of having a safer, easily replenished source of red blood cells was made possible using human endometrium derived iPSCs for the first time. The concept of preserving a self-driven pluripotent cell source that can be indefinitely maintained and expanded has opened numerous possibilities in tissue engineering.(26, 27) Hematopoietic and other blood progenitors with various end-points have been derived from either skin fibroblast-driven iPSCs, cord blood, or peripheral blood mononuclear cells.(28–32) Although the derivation of erythroid lineage cells has been previously attempted by other scholars,(1, 2) a reliable, full spectrum RBC differentiation protocol from discarded endometrial tissue after hysterectomy has been established.
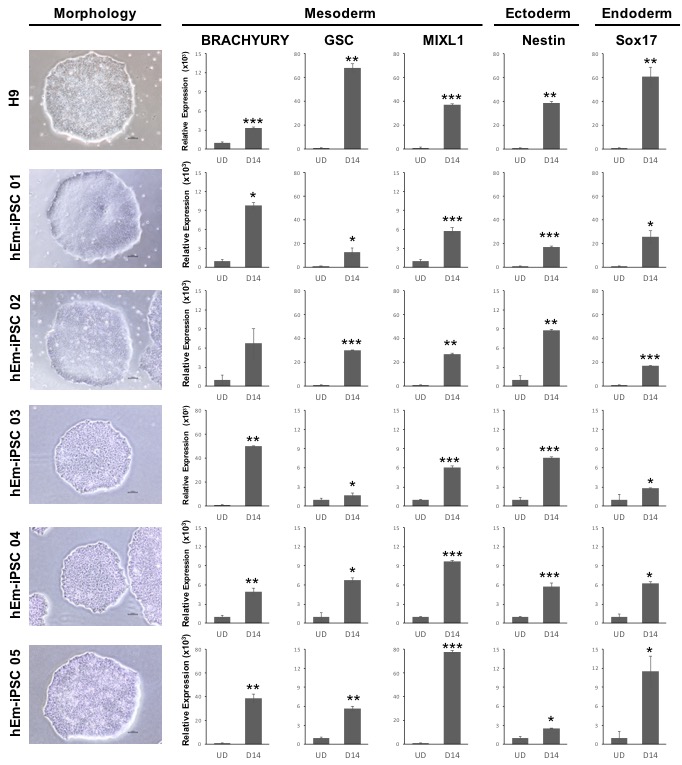
In this study, hEm-iPSCs were established from human endometrial cells using episomal iPSC reprogramming vectors (Oct4, Sox2, KFL4, L-Myc, Lin28), which constitutes a transgene-free and virus-free system.(10, 11) hEm-iPSCs were produced and maintained using a feeder-free culture system, and the characteristics of the dedifferentiated stem cell line were confirmed by differentiation into three germ layers. A stepwise strategy involving both feeder and feeder-free conditions was employed for erythroid differentiation to achieve better differentiation efficiency compared to other protocols.(33) Murine bone marrow stromal fibroblasts have been previously utilized to support hematopoietic commitment by providing the appropriate in vitro milieu, where the components cannot be fully replaced in feeder-free conditions. Such feeder condition was used in our protocol for robust commitment to hematopoiesis. Consequently, cocktails of specific growth factors could be used to induce in vitro hematopoiesis,(34) which optimized through this study.
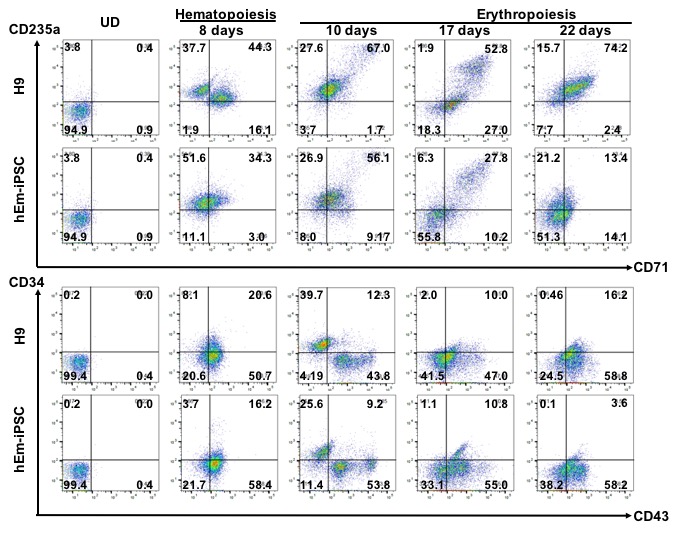
Other groups have attempted various CD34 + cell-driven, neural stem cell-driven, and fibroblast-driven iPSCs, claiming that the differentiation efficiency of CD43 + cells is similar regardless of donor origin when differentiation is achieved via embryoid body (EB) formation, with efficiencies slightly below 20%.(29, 35) Although our system used a shortened 2 day, two phase EB protocol, the rate of CD43 + cells using human endometrium-derived iPSCs was between 60% and 70% only after an 8 days of culture, before erythroid commitment was induced. Unlike ES cells, iPSCs are known to possess epigenetic memory of the donor cell; therefore, the efficiency of directed differentiation was reported to be lowered in some studies and not in others 37, 38. Such impairment in differentiation becomes attenuated as the iPSCs are passed beyond passage 15, (36–39) a characteristic that provides hindrance with regards to time and efficiency. Cells between 20 and 30 passages for hEm-iPSCs, and between 42 and 50 for H9 were used for the differentiation process in the current study.
According to the Flow cytometric analyses and Giemsa differential counting, the conversion from hematopoietic stem cells to the erythroid fate is more efficient in the hEm-iPSCs compared to the H9 control, the mechanisms of which warrants further analysis. Moreover, the cell source originates from tissue which would otherwise be discarded after pathologic examination, is abundant and easily propagated in vitro.
The hallmark of a successful erythroid differentiation is the confirmation of the in vitro oxygen-carrying capacity of the final product, which shows that the differentiated erythroblasts can produce hemoglobin with oxygen binding and dissociation abilities similar to that of peripheral blood. Further studies required as an extension of this study is to polish the enucleation process of the normoblasts, and the other blood components including white blood cells and platelet formation could be attempted to be used in tailored in vitro disease modelling. In this study, the enucleation rate, which is the possible stage of blood transfusion, was below 10%, and the enucleation of mature RBCs from iPSCs and ESCs has not yet been resolved.(40) Primitive tissues that appear in early embryogenesis are the most suitable preliminary targets for iPS or ES cell differentiation in the field of regenerative medicine, as the signals and environment involved in more complex terminally differentiated tissues are still poorly understood and also require further studies.
{kind=link}
{kind=link}