Several approaches have been evaluated for the management of chemotherapy-induced cardiotoxicity. Some prophylactic and chemoprotective agents such as dexrazoxane, statins, cyclooxygenase inhibitors, beta-blockers, angiotensin antagonists, diuretics, spironolactone, digoxin and erythropoietin are reported to be somewhat effective to reduce cardiotoxicity [8, 24]. However, prevention of cardiotoxicity remains a major problem in cancer patients and recent investigations have focused on natural compounds.
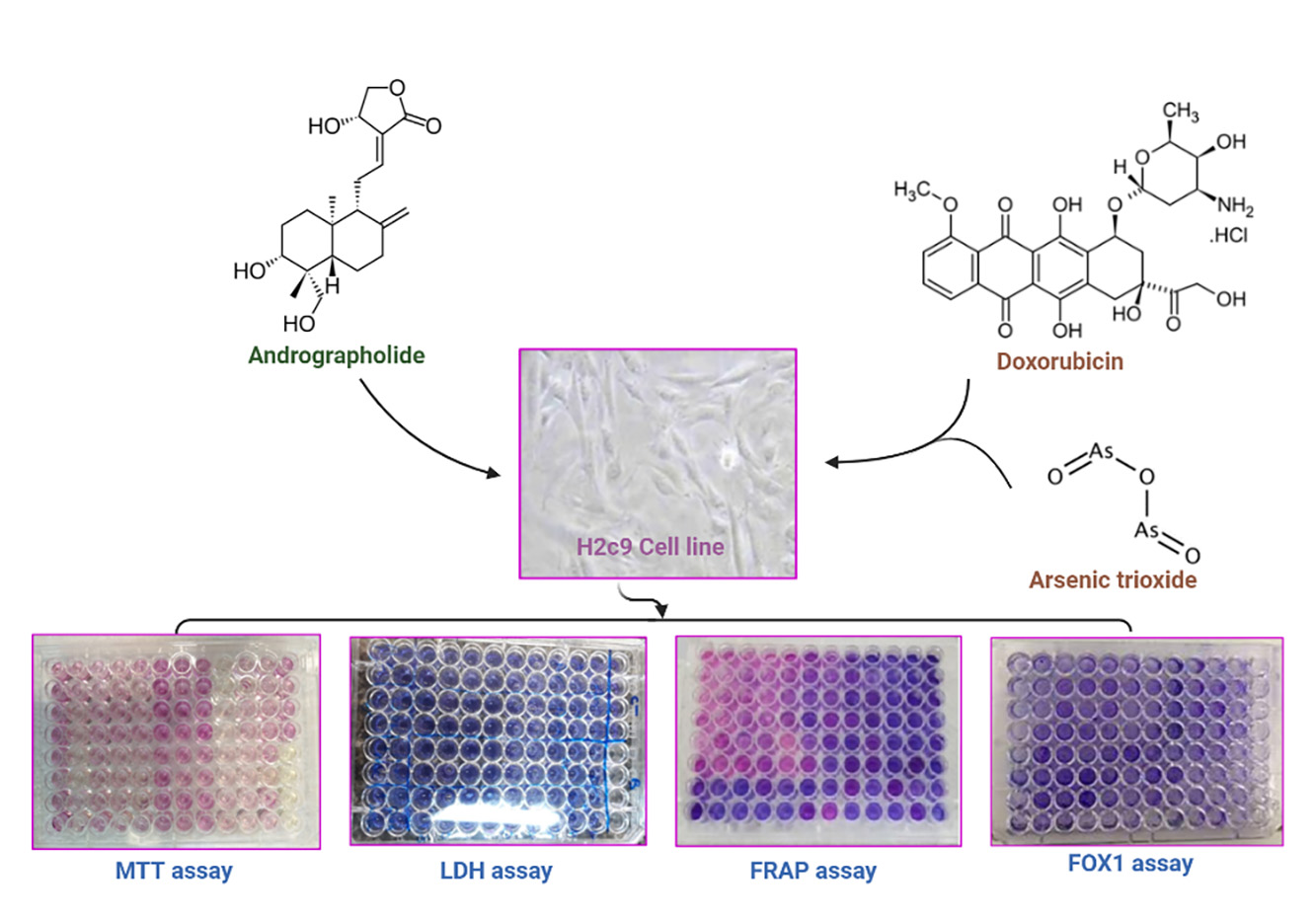
In the present investigation, in vitro evaluation of AG as a bioactive agent revealed cytoprotective and antioxidant activities against toxicities caused by DOX and ATO in H9C2 cells through raising the cellular viability and FRAP value, and lessening the cytotoxicity, hydroperoxides concentration and TLR4 expression.
In our study, the MTT cell viability assay presented non-inhibitory effect of AG at the concentration range of 1–10 µM on H9C2 cells after 24 h treatment however there was a significant reduction in cell viability at the concentration of 40 µM. AG markedly prevented the cytotoxicity caused by DOX and ATO at the concentrations of 2.5, 5 and 10 µM.
In the study of Woo et al, AG at the concentrations of 1, 3 and 10 µM had no obvious effect on the viability of neonatal rat cardiomyocyte and showed protective activity against cellular injury caused by hypoxia/reoxygenation in LDH release test [18]. Dey et al also evaluated AG at the range of 2.5–40 µM concentrations in liver cancerous and non-cancer cell lines and reported the viability percentage as 90% after incubation with 20 µM AG and IC50 value of more than 40 µM in non-cancer cell lines [25]. In another study, AG showed anti-apoptotic effect at the concentrations of 1, 5, and 10 µM in H9C2 cells during high glucose condition through alleviating caspase-3 activity and Bax/Bcl-2 ratio [26]. However, Wu et al reported that AG did not disturb cardiomyocyte viability at the concentrations of 12.5, 25 or 50 µM using the cell counting kit assay-8 and it significantly prohibited the cytotoxicity induced by Ang II [27]. They reported that 7-weeks treatment with AG reduced heart dysfunction and diminished fibrosis and hypertrophy through down regulation of expression of atrial natriuretic peptide, brain natriuretic peptide, transforming growth factor β, connective tissue growth factor, collagen I and III genes in a mouse model of cardiac hypertrophy. In their study, AG also protects cardiomyocytes against hypertrophic changes induced by angiotensin II via suppressing mitogen-activated protein kinases (MAPKs) pathway [27].
The protective effects of AG against some cardiac disorders have similarly been described in several investigations. In myocardial infarction, AG has shown protective activity against heart remodeling via augmenting the Nrf2 pathway [17]. AG has dampened myocardial dysfunction caused by lipopolysaccharide in mice through suppressing phosphorylation of IκB and activation of NF-κB and hindering synthesis of NO and inflammatory markers such as TNF-α and IL-1ß, and apoptosis of cardiac cells (28). In diabetic cardiomyopathy, AG has been able to inhibit oxidative, inflammatory and apoptotic changes and consequently improved hypertrophy and fibrosis in heart tissue [26].
Furthermore, our data displayed lessening in hydroperoxides content and noteworthy raising in FRAP value in H9C2 cells after incubation with AG confirming its potent antioxidant properties. The mechanisms associated with anti-oxidative activities of AG are as follows: maintaining the integrity of mitochondrial, counteracting free radicals, reducing ROS formation via inhibition of nicotinamide adenine dinucleotide phosphate (NADPH) oxidase and iNOS and inactivation of NF-κβ signaling pathway, scavenging of several free radicals such as 1,1-diphenyl-2-picrylhydrazyl (DPPH) and hydroxyl radicals, increasing NF-E2–related factor 2 (Nrf2) and heme oxygenase-1 (HO-1) activity [29]. Previous studies have also shown that treatment of cardiomyocytes with AG has enhanced the cellular glutathione stores and the activities of enzymes including superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase and hence the heart antioxidant defense [18, 26].
Moreover, our findings revealed that AG can attenuate the expression of TLR4 gene in cardiotoxicity caused by DOX and ATO. There are several documents for the contribution of TLR2 and TLR4 overexpression in the pathogenesis of heart toxicity in response to DOX [8, 30]. TLR4 activity is also increased in other heart pathology such as hypertension or heart failure and is linked with oxidative stress, inflammatory and fibrotic pathways [31].
Unlike DOX, little data has been described for the role of TLR overexpression in ATO-induced cardiomyopathy. In a recent article, Zheng et al reported that ATO-induced cardiac injury was related to the stimulation of TLR4/NF-κB signaling and inflammatory reactions [32].
Instead, various analogs of AG have shown powerful anti-inflammatory properties through suppression of TLR4/NF-κB pathways (33). AG also has shown anticancer activity via inhibitory action on TLR4/NF-κB system in some cancerous cells and tumors [19, 34].
{kind=link}